
“Findings in the literature suggest that prompt surgical treatment of patients with fulminant Clostridium difficile-associated disease (CDAD) is necessary to ensure patient survival. However, controversy remains regarding the best surgical approach and timing. Recent efforts have been made in the creation of a scoring system to predict deterioration and improve patient care. New surgical approaches such as ileostomy and washout have shown promising results, but more rigorous data and longer follow-up, especially with regard to
disease recurrence after ileostomy reversal, are needed to evaluate the true value of these techniques regarding mortality.”
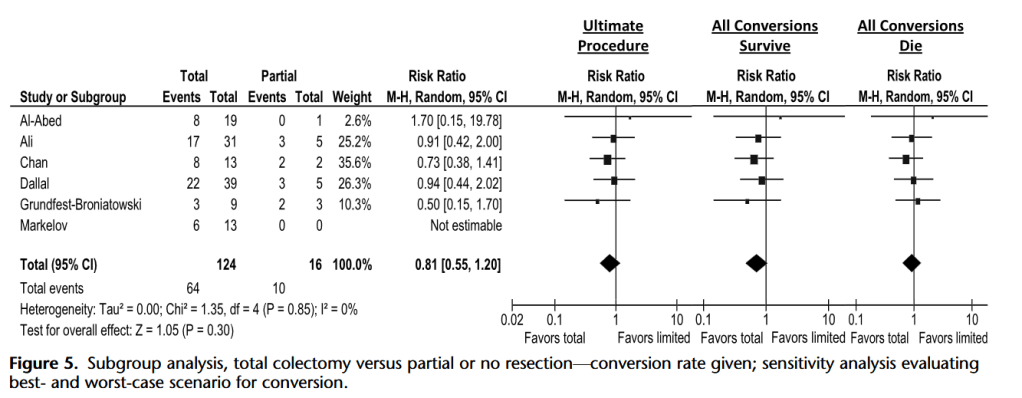
“In the worst-case scenario with the given data, total colectomy does not increase mortality. In the best-case scenario with the given data, total colectomy may decrease mortality. Many of the patients who ultimately died after total colectomy had significant delay in this procedure, with many first undergoing a more limited procedure, thus blunting the effectiveness of the total colectomy and making our positive estimate likely too conservative. In addition, in each of the studies, the proportion of patients undergoing less than a total
colectomy is quite small. This likely reflects selection bias. Most of the studies suggest that the patients were quite different, with the patients undergoing total colectomy being much sicker, with having more comorbidities, thus having a higher baseline mortality.”
Ferrada, Paula et al. “Timing and type of surgical treatment of Clostridium difficile-associated disease: a practice management guideline from the Eastern Association for the Surgery of Trauma.” The journal of trauma and acute care surgery vol. 76,6 (2014): 1484-93. Full Text for Emory Users
