
Liu R, Wang J, Zhao G, Su Z. Negative pressure pulmonary edema after general anesthesia: A case report and literature review. Medicine (Baltimore). 2019 Apr;98(17): e15389. doi: 10.1097/MD.0000000000015389.
It is widely accepted that the central mechanism of postoperative NPPE is related to rapid negative intrapleural pressure increasing due to forceful inspiration against the obstruction, which can be up to 10 times or more that of normal breathing. [7] A typical event leading to acute airway obstruction associated with postoperative NPPE is laryngospasm. Other procedure that increases the risk of NPPE includes oropharyngeal, head, and neck surgery. Five [8–12] of the reported 29 cases involved upper respiratory tract surgery, and 10 [1,3,6,7,13–18] of the cases involved head and neck surgery, which may be related to tissue swelling and the sensitive dilator muscle of the upper airway in head and neck surgeries.
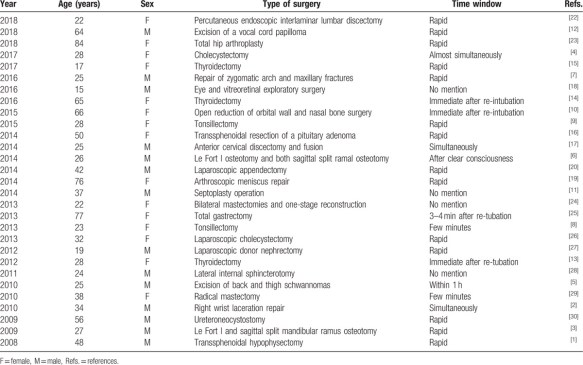
Table 1. Reported cases of negative pressure pulmonary edema from 2008 to 2018.
Bhattacharya M, Kallet RH, Ware LB, Matthay MA. Negative-Pressure Pulmonary Edema. Chest. 2016 Oct;150(4):927-933. doi: 10.1016/j.chest.2016.03.043.
In adults, airway obstruction leading to NPPE is most often reported in the context of postextubation laryngospasm following surgery.6 The incidence of NPPE following laryngospasm is difficult to compute from case series data, although one study derived from the Australian Incident Monitoring Study (AIMS) reported 189 cases of laryngospasm in 4,000 anesthesia adverse events.10 There were five cases of NPPE, an incidence of 3% of those with laryngospasm. This statistic may overestimate the true incidence of NPPE, as reporting of cases in AIMS is voluntary and likely favors severe presentations over milder episodes of laryngospasm. Indeed, other estimates of the incidence of NPPE have ranged as low as 0.1% of laryngospasm cases. [11] Of note, one study reported a higher incidence of NPPE among men (80% of NPPE cases) following laryngospasm, and in patients categorized as ASA (American Society of Anesthesiologists) status I or II (73% of NPPE cases). The authors postulate that this finding may relate to higher negative thoracic pressures achieved by healthy male patients. [11]
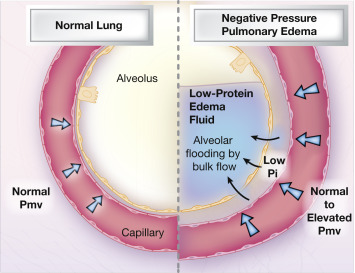
Figure 2. The alveolocapillary unit. In health (left), the alveolus remains fluid-free, because liquid filtered by Starling transcapillary forces is cleared by interstitial lymphatics. In negative-pressure pulmonary edema (right), negative interstitial pressure results in an increased hydrostatic gradient and alveolar flooding. The afterload-increasing effect of the Müller maneuver increases this gradient because of elevated left ventricular, left atrial, and thus pulmonary capillary pressures. Pi = interstitial pressure; Pmv = microvascular pressure.
See also: Kao CL, Kuo CY, Su YK, Hung KC. Incidence of negative-pressure pulmonary edema following sugammadex administration during anesthesia emergence: A pilot audit of 27,498 general anesthesia patients and literature review. J Clin Anesth. 2020 Jan 14;62:109728. doi: 10.1016/j.jclinane.2020.109728. [Epub ahead of print]
Full-text for Emory users.
More PubMed results on NPPE.
