
“Emergency Department visits and hospital readmission after thyroidectomy are common, and there are several practices that can reduce their occurrence. Routine postoperative calcium and vitamin D supplementation may reduce rates of postoperative hypocalcemia, and avoiding postoperative hypertension may decrease the risk of neck hematoma development and the need for reoperation. Older age, thyroid cancer, dependent functional status, higher ASA score, diabetes, chronic obstructive pulmonary disease, steroid use, hemodialysis, and recent weight loss increase the risk of hospital readmission after thyroid surgery. By further identifying risk factors for reoperation, ED visits, and readmission, this review may assist practitioners in optimizing perioperative care and therefore reducing patient morbidity and mortality after thyroid operations.”
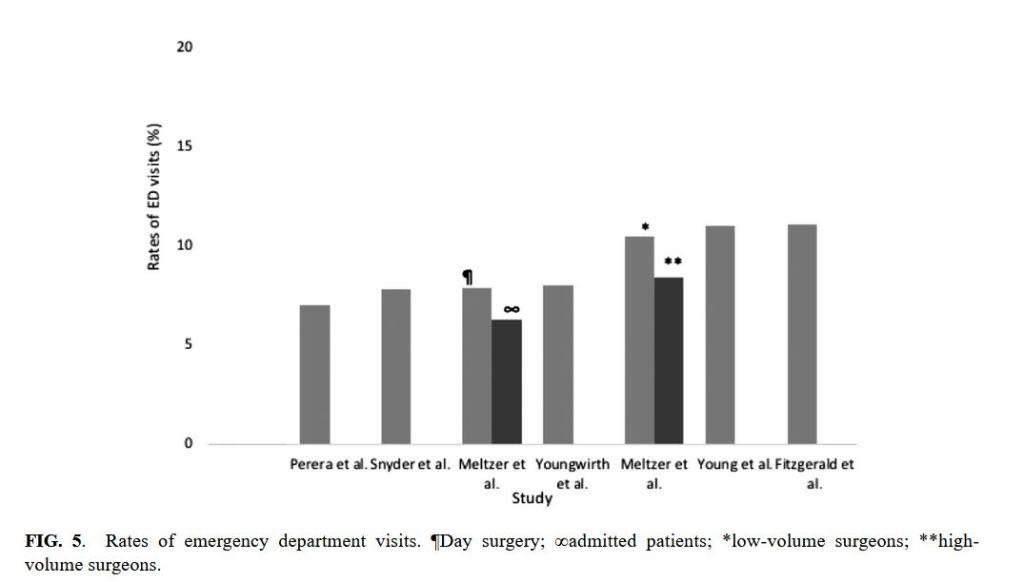
“In summary, the pooled rates of reoperation, ED visits, and unplanned hospital readmissions were 0.6%, 8.1%, and 2.7%, respectively. Factors that increase the risk of post-thyroidectomy hospital readmission include total thyroidectomy, African American race/ethnicity, diabetes, chronic kidney disease requiring hemodialysis, chronic obstructive pulmonary disease, steroid use, dependent functional status, thyroid cancer, recent weight loss, obesity, BMI <18.6 kg/m2, bleeding disorders, liver disease, hypoalbuminemia, and previous surgery within 30 days. This literature review identified several strategies that could potentially reduce readmission and ED visits. First, it is advised that extra caution should be exercised when performing a thyroidectomy on individuals with the aforementioned risk factors for hospital readmission. Similarly, identifying patients at risk for hematoma development is important when determining who is suitable for outpatient surgery. When possible, all anticoagulant and antithrombotic medication should be discontinued prior to surgery, but this should be discussed first with relevant subspecialists. Decisions regarding VTE prophylaxis should be individualized, but in general there is no need for routine UFH or LMWH in most thyroidectomy patients, unless they are at the highest risk for VTE. Reducing postoperative hypertension may also prove beneficial in reducing postoperative hematoma and reoperation risk. In order to reduce hypocalcemia-related ED visits and hospital readmissions, routine postoperative hypoparathyroidism prevention with 2–3 g of oral calcium daily, as well as activated vitamin D supplementation for at least two to three weeks, is recommended. Lastly, attention should be paid to patient education, and when possible, explicit written instructions specifying when to seek emergency care should be provided to patients.”
Margolick, Joseph et al. “Systematic Review and Meta-Analysis of Unplanned Reoperations, Emergency Department Visits and Hospital Readmission After Thyroidectomy.” Thyroid : official journal of the American Thyroid Association vol. 28,5 (2018): 624-638. Full Text for Emory Users
