
“Afferent loop obstruction is a purely mechanical complication that infrequently occurs following construction of a gastrojejunostomy. The operations most commonly associated with this complication are gastrectomy with Billroth II or Roux-en-Y reconstruction, and
pancreaticoduodenectomy with conventional loop or Roux-en-Y reconstruction. Etiology of afferent loop obstruction includes:
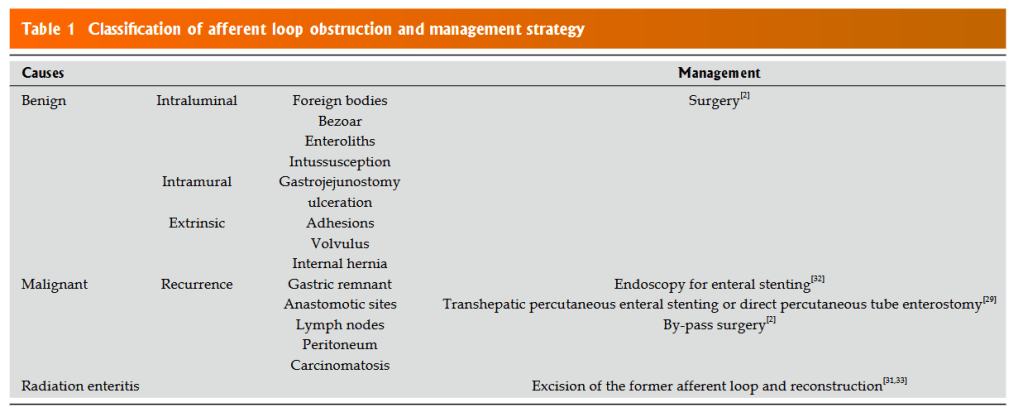
(1) entrapment, compression and kinking by postoperative adhesions
(2) internal herniation, volvulus and intussusception
(3) stenosis due to ulceration at the gastrojejunostomy site and radiation enteritis of the afferent loop
(4) cancer recurrence
(5) enteroliths, bezoars and foreign bodies.
“Creation of a gastrojejunostomy leaves a segment of proximal small bowel, most commonly consisting of duodenum and proximal jejunum, lying upstream from the gastrojejunostomy. This limb of intestine conducts bile, pancreatic juices, and other proximal intestinal secretions toward the gastrojejunostomy and is termed the afferent loop. Afferent loop obstruction (ALO) is a purely mechanical complication that infrequently occurs following
construction of a gastrojejunostomy. The operations most commonly associated with this complication include total gastrectomy with loop esophagojejunostomy and simple
or pouch Roux-en-Y reconstruction, partial gastrectomy with Billroth II and Roux-en-Y reconstruction, and pancreaticoduodenectomy with conventional loop and
Roux-en-Y reconstruction performed for treatment of benign and malignant causes.”
Blouhos, Konstantinos et al. “Management of afferent loop obstruction: Reoperation or endoscopic and percutaneous interventions?.” World journal of gastrointestinal surgery vol. 7,9 (2015): 190-5. Free Full Text
