
One discussion this week focused on pelvic drains.
Reference: Denost Q, et al. To drain or not to drain infraperitoneal anastomosis after rectal excision for Cancer: The GRECCAR 5 randomized trial. Annals of Surgery. 2017 Mar;265(3):474-480. doi:10.1097/SLA.0000000000001991.
Summary: The GRECCAR 5 randomized trial sought to explore the benefit of a drain for postoperative pelvic sepsis, overall morbidity and mortality, rate of re-operation, length of stay, and rate of stoma closure at 6 months (p.474). It involved 469 patients (236 with drains, 233 without) between 2011 and 2014.
Ultimately, the trial did not find any benefit of the pelvic drain after low anterior resection for rectal cancer. Thus, the authors “recommend not using pelvic drain after rectal excision for cancer, except in case of operative bleeding or beyond TME surgery” (p.480).
The drain did not contribute to an efficient diagnosis of sepsis, for the time to diagnosis of pelvic sepsis was an average of 7.8 days, yet the drain was removed at 5.5 days postop (see figure below; p.1478).
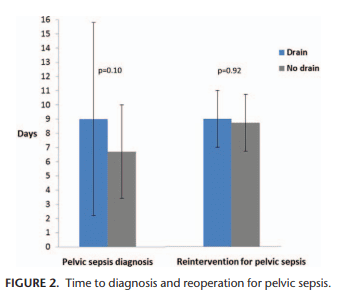
There was no significant difference between the two groups for any of the noted measurements. Pelvic sepsis occurred in 16.1% of those with the drain and 18.0% of those without drain. Re-operation for pelvic sepsis was done in 10.2% of those with drain and 12.0% of those without drain.
Additional reading: Placer C. To drain or not to drain infraperitoneal anastomosis after rectal excision for cancer: an unclosed debate [Letter to the Editor]. Annals of Surgery. 2018. doi:10.1097/SLA.0000000000003005. [Epub ahead of print]
