
One discussion this week included a trial out of Denmark comparing D1 and D2 lymph-node dissection for gastric cancer.
Reference: Bonenkamp JJ, et al. Extended lymph-node dissection for gastric cancer. NEJM. 1999 Mar 25;340(12):908-914.
Summary: Curative resection is the treatment of choice for gastric cancer, but it is unclear whether this operation should include an extended (D2) lymph-node dissection or a limited (D1) dissection. The authors conducted a randomized trial in 80 Dutch hospitals in which they compared D1 with D2 lymph-node dissection for gastric cancer in terms of morbidity, postoperative mortality, long-term survival, and cumulative risk of relapse after surgery.
Between August 1989 and July 1993, 996 patients were enrolled. Of these, 711 underwent randomly assigned treatment (D1 = 380, D2 = 331) and 285 received palliative treatment.
General findings:
- Complications: 43% in D2, 25% in D1
- Postoperative deaths: 10% in D2, 4% in D1
- Length of stay: 16 median days in D2, 14 days in D1
- 5-year survival rates: 47% in D2, 45% in D1
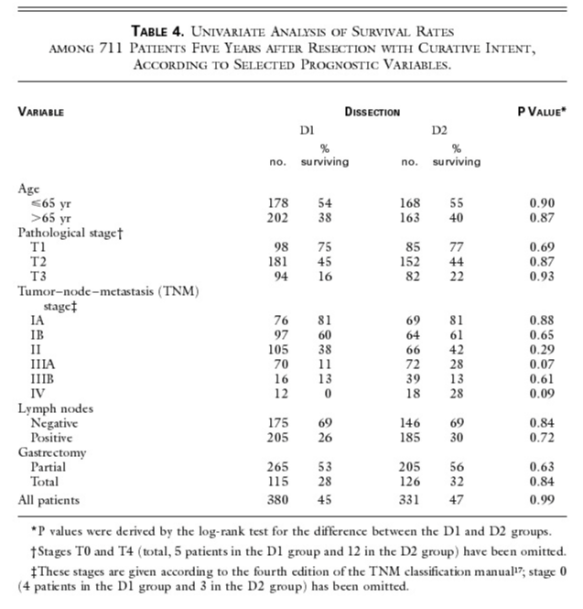
One of the arguments for D2 dissection is its ability to reduce rates of local recurrence, thereby increasing the quality of life. The distressing finding of local recurrence, usually in a terminal phase of the disease, often leads to second operations to restore gastrointestinal continuity. In this trial, there was a tendency toward a reduced cumulative risk of relapse after D2 dissection, but the rate of relapse remained high and the difference from D1 dissection was not significant. A subgroup analysis indicated a significant or marginally significant difference for patients with disease in UICC stages II and IIIA, but this difference was attributable largely to stage migration.
