“Tranexamic acid (TXA) is an antifibrinolytic agent that competitively inhibits the conversion
of plasminogen to plasmin. TXA is also believed to have an anti-inflammatory effect and may improve platelet function under certain circumstances. TXA has increasingly gained recognition in perioperative use to mitigate the risk of postoperative bleeding. Originating in the field of anesthesiology, TXA is used to control surgical, traumatic, and postpartum hemorrhage. Meanwhile, perioperative TXA administration has been established in orthopedic and cardiothoracic surgery. It is also becoming popular in plastic surgery, especially regarding craniomaxillofacial procedures. Although the evidence on
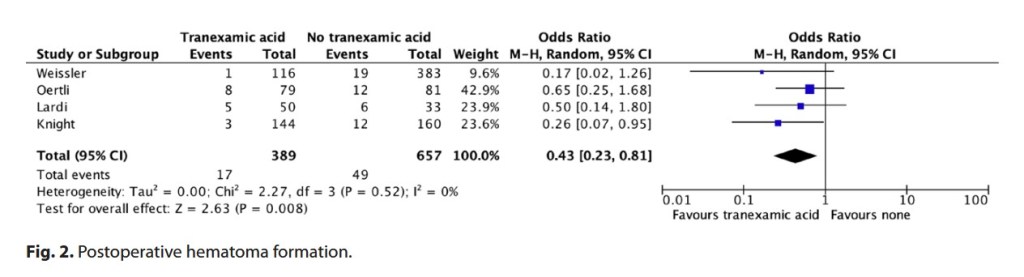
the use of TXA in breast surgery is improving, its value still needs further investigation.”