
Poris S, et al. Routine versus selective upper gastrointestinal contrast series after omental patch repair for gastric or duodenal perforation. Surg Endosc. 2018 Jan; 32(1):400-404.
Full-text for Emory users.
“Age greater than 60 years (p-0.0470, CI-0.76-31.54), pulse rate greater than 110/minute (p-0.0217, CI-1.04-34.48), systolic blood pressure less than 90 mm Hg (p-0.0016, CI-2.04-71.9), haemoglobin level less than 10 g/dl (p-0.0009, CI-2.25-135.02), serum albumin less than 2.5 grams/dl (p-0.0145, CI-1.21-38.31), total lymphocyte count less than 1800 cells/mm-3 (p-0.0003, CI-8.9-42.2), size of perforation greater than 5 mm (p-0.0011, CI-1.09-36.13) were identified as risk factors for releak. Serum albumin, hemoglobin and size of perforation were independent risk factors for prediction of releak on multivariate analysis. The anthropometric parameters namely mean triceps skin fold thickness, mean mid arm circumference and mean body mass index were all significantly less in cases as compared to controls. Releak was found to be a significant cause of death in patients with perforated duodenal ulcer. A total of 8 patients died in both the groups. The mortality rate in the releak group was 55.6% (5 out of 9 patients) compared to 2.7% (3 out of 110 patients) in the control group [p-0.0001].”
Gupta S, et al. The management of large perforations of duodenal ulcers. BMC Surg. 2005 Jun 25;5:15.
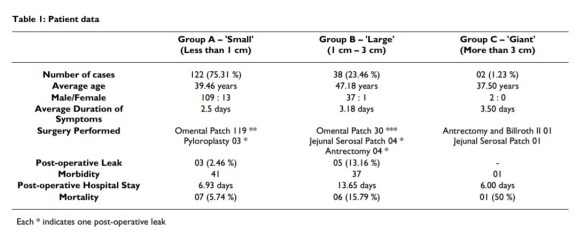
“The results of omentopexy in small and large sized perforations in the present series give statistically similar results. The leak rates and mortality of the two groups after omentopexy remain comparable, thereby suggesting that this may be considered as the procedure of choice in all perforations up to a size of 3 cms. The procedure is simple and easy to master, and, avoids the performance of a major resection in a patient who is already compromised. In fact, Sharma et al also reported the success of the omental plug in perforations of duodenal ulcers more than 2.5 cms in size; only, they preferred using a free graft of the omentum rather than a pedicled one [6]. We feel that mobilization of the omentum on its pedicle from the colon, and placement of sutures into the normal duodenum away from the perforation makes the performance of omental patch safe even in the presence of large sized perforations.”
Kumar K, et al. Factors contributing to releak after surgical closure of perforated duodenal ulcer by Graham’s Patch. Trop Gastroenterol. 2002 Oct-Dec;23(4):190-2.
Emory users, request full-text article here.
“Age greater than 60 years (p-0.0470, CI-0.76-31.54), pulse rate greater than 110/minute (p-0.0217, CI-1.04-34.48), systolic blood pressure less than 90 mm Hg (p-0.0016, CI-2.04-71.9), haemoglobin level less than 10 g/dl (p-0.0009, CI-2.25-135.02), serum albumin less than 2.5 grams/dl (p-0.0145, CI-1.21-38.31), total lymphocyte count less than 1800 cells/mm-3 (p-0.0003, CI-8.9-42.2), size of perforation greater than 5 mm (p-0.0011, CI-1.09-36.13) were identified as risk factors for releak. Serum albumin, hemoglobin and size of perforation were independent risk factors for prediction of releak on multivariate analysis. The anthropometric parameters namely mean triceps skin fold thickness, mean mid arm circumference and mean body mass index were all significantly less in cases as compared to controls. Releak was found to be a significant cause of death in patients with perforated duodenal ulcer. A total of 8 patients died in both the groups. The mortality rate in the releak group was 55.6% (5 out of 9 patients) compared to 2.7% (3 out of 110 patients) in the control group [p-0.0001].”
