
Pislaru SV, et al. Aortic stenosis and noncardiac surgery: managing the risk. Curr Probl Cardiol. 2015 Nov;40(11):483-503.
Full-text for Emory users.
“In summary, the mortality risk at contemporary noncardiac surgery has followed the general trend of decreasing surgical mortality rate, and is currently at 1.5%-4% for elective procedures, significantly lower than those in the early reports (Fig 1). Presence of severe AS does not result in increased mortality rates, but rather in excess cardiovascular morbidity (most notably myocardial infarction [13] or new or worsening heart failure [14]). Symptomatic patients have worse outcomes.” (pg. 488)
 FIG 3. Proposed algorithm for managing patients with severe AS in need of noncardiac surgery. Emergency noncardiac surgery (NCS) obviously needs to be performed without consideration of the AS; these patients are at the highest risk of perioperative morbidity and mortality. Aortic balloon valvuloplasty (ABV) can be considered in patients needing urgent noncardiac surgery; transcatheter aortic valve replacement (TAVR) is an alternative, but the necessary assessment of vascular access and LVOT sizing cannot usually be performed in due time. Asymptomatic patients can in general proceed with elective noncardiac surgery; however, surgical aortic valve replacement (SAVR) or TAVR should be considered before high-risk surgical interventions, or in patients with revised cardiac risk index (RCRI) ≥2. Symptomatic patients should in general undergo TAVR or SAVR before noncardiac surgery, unless the need for antithrombotic therapy required after TAVR or SAVR unduly delays or increases the risk of noncardiac surgery, or when the noncardiac surgery could decrease the risk of anticipated SAVR or TAVR for severe symptomatic aortic stenosis. Concomitant SAVR and noncardiac surgery can also be considered in selected patients (see the text for details). LVOT, left ventricular outflow tract.
FIG 3. Proposed algorithm for managing patients with severe AS in need of noncardiac surgery. Emergency noncardiac surgery (NCS) obviously needs to be performed without consideration of the AS; these patients are at the highest risk of perioperative morbidity and mortality. Aortic balloon valvuloplasty (ABV) can be considered in patients needing urgent noncardiac surgery; transcatheter aortic valve replacement (TAVR) is an alternative, but the necessary assessment of vascular access and LVOT sizing cannot usually be performed in due time. Asymptomatic patients can in general proceed with elective noncardiac surgery; however, surgical aortic valve replacement (SAVR) or TAVR should be considered before high-risk surgical interventions, or in patients with revised cardiac risk index (RCRI) ≥2. Symptomatic patients should in general undergo TAVR or SAVR before noncardiac surgery, unless the need for antithrombotic therapy required after TAVR or SAVR unduly delays or increases the risk of noncardiac surgery, or when the noncardiac surgery could decrease the risk of anticipated SAVR or TAVR for severe symptomatic aortic stenosis. Concomitant SAVR and noncardiac surgery can also be considered in selected patients (see the text for details). LVOT, left ventricular outflow tract.
Agarwal S, et al. Impact of aortic stenosis on postoperative outcomes after noncardiac surgeries. Circ Cardiovasc Qual Outcomes. 2013 Mar 1;6(2):193-200.
Methods and Results: Patients undergoing NCS with moderate AS (valve area: 1.0–1.5 cm2) or severe AS (valve area: <1.0 cm2) were identified using the surgical and the echocardiographic databases. Using propensity score analysis, we obtained 4 matched control patients without AS for each patient with AS undergoing NCS. The propensity score matching used the 6 revised cardiac risk index criteria, in addition to age and sex. Primary outcome was a composite of 30-day mortality and postoperative myocardial infarction. We matched 634 patients with AS undergoing NCS to 2536 controls. There were 244 patients with severe AS and 390 patients with moderate AS. Thirty-day mortality was 2.1% for AS patients compared with 1.0% in non-AS controls (P=0.036). Postoperative myocardial infarction was more frequent in patients with AS compared with controls (3.0% versus 1.1%; P=0.001). Combined primary outcome was significantly worse for both moderate and severe AS patients compared with respective controls (4.4% versus 1.7%; P=0.002; and 5.7% versus 2.7%; P=0.02, respectively). High-risk surgery, symptomatic severe AS, coexisting mitral regurgitation, and preexisting coronary disease were significant predictors of primary outcome in patients with AS.
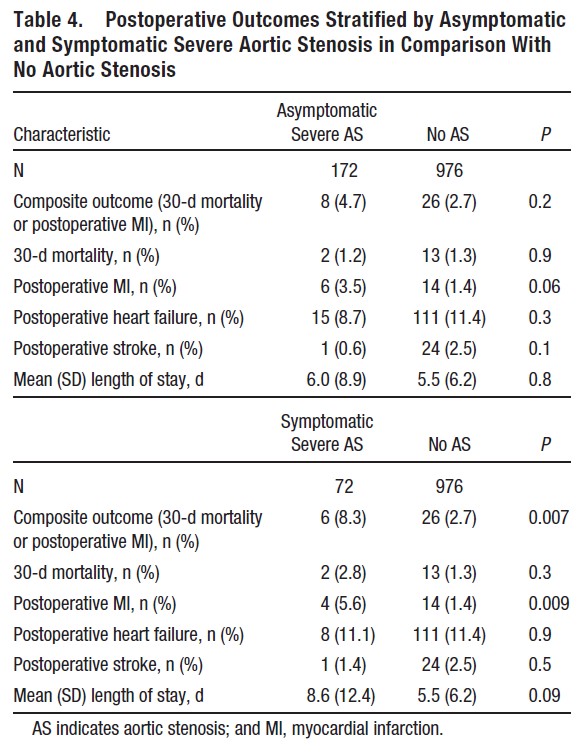 Table 4. gives the postoperative outcomes in the severe AS group stratified by presence or absence of symptoms at the time of preoperative screening compared with the outcomes in the corresponding non-AS population. In comparison with the non-AS group (2.7%), the incidence of primary outcome was significantly higher in the symptomatic severe AS group (8.3%; P=0.007). The difference in primary outcome was largely attributable to the higher incidence of postoperative MI in the symptomatic severe AS group (5.6%) as compared with the non-AS group (1.4%; P=0.009).
Table 4. gives the postoperative outcomes in the severe AS group stratified by presence or absence of symptoms at the time of preoperative screening compared with the outcomes in the corresponding non-AS population. In comparison with the non-AS group (2.7%), the incidence of primary outcome was significantly higher in the symptomatic severe AS group (8.3%; P=0.007). The difference in primary outcome was largely attributable to the higher incidence of postoperative MI in the symptomatic severe AS group (5.6%) as compared with the non-AS group (1.4%; P=0.009).
More PubMed results on patients with aortic stenosis undergoing noncardiac surgery.
