Lak KL, Goldblatt MI. Mesh Selection in Abdominal Wall Reconstruction. Plast Reconstr Surg. 2018 Sep;142(3 Suppl):99S-106S. Full-text for Emory users.
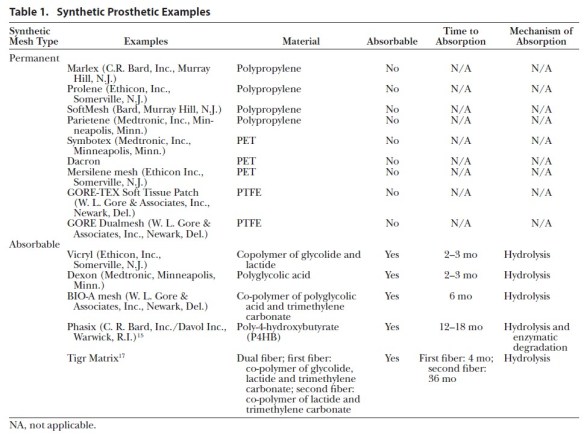

Lak KL, Goldblatt MI. Mesh Selection in Abdominal Wall Reconstruction. Plast Reconstr Surg. 2018 Sep;142(3 Suppl):99S-106S. Full-text for Emory users.
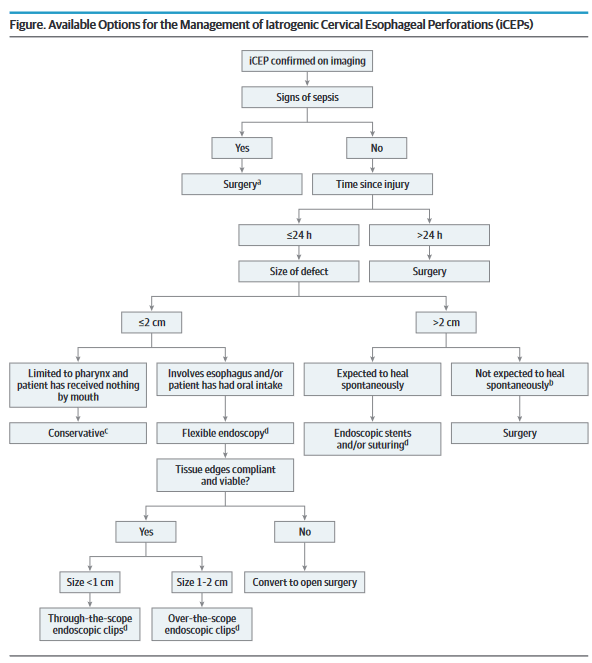
“Esophageal perforations are difficult to diagnose and have a high mortality rate. The existing studies on esophageal perforations address treatment by anatomic location and by cause, but few focus specifically on iCEPs. The management of iCEPs is controversial. There is a need for additional prospective studies comparing treatment options for iCEPs to establish a gold standard treatment and to assess for the expanding role of endoscopic interventions.” (Chen)
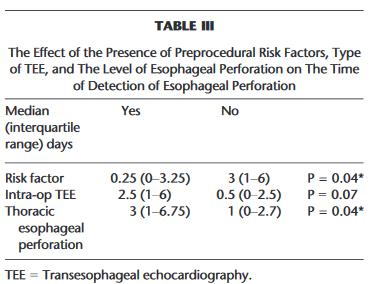
“Transesophageal echocardiography (TEE) is a commonly performed procedure, either in an
intra-operative setting of a cardiac surgical procedure or a nonoperative setting, such as to evaluate for an intracardiac thrombi.”
No. Because of its properties, it will render an abdomen impossible to re-enter for a minimum of 3 months. Should you have a need to reenter the abdomen within the ten-day window that surgeons have traditionally considered safe for abdominal re-entry, placement of VICRYL® mesh will render the abdomen ‘hostile’ for a minimum of three months.
Continue readingNovitsky YW, Elliott HL, Orenstein SB, Rosen MJ. Transversus abdominis muscle release: a novel approach to posterior component separation during complex abdominal wall reconstruction. Am J Surg. 2012 Nov;204(5):709-16.
Full-text for Emory users.
Background: Several modifications of the classic retromuscular Stoppa technique to facilitate dissection beyond the lateral border of the rectus sheath recently were reported. We describe a novel technique of transversus abdominis muscle release (TAR) for posterior component separation during major abdominal wall reconstructions.
Methods: Retrospective review of consecutive patients undergoing TAR. Briefly, the retromuscular space is developed laterally to the edge of the rectus sheath. The posterior rectus sheath is incised 0.5-1 cm underlying medial to the linea semilunaris to expose the medial edge of the transversus abdominis muscle. The muscle then is divided, allowing entrance to the space anterior to the transversalis fascia. The posterior rectus fascia then is advanced medially. The mesh is placed as a sublay and the linea alba is restored ventral to the mesh.
Continue readingPislaru SV, et al. Aortic stenosis and noncardiac surgery: managing the risk. Curr Probl Cardiol. 2015 Nov;40(11):483-503.
Full-text for Emory users.
“In summary, the mortality risk at contemporary noncardiac surgery has followed the general trend of decreasing surgical mortality rate, and is currently at 1.5%-4% for elective procedures, significantly lower than those in the early reports (Fig 1). Presence of severe AS does not result in increased mortality rates, but rather in excess cardiovascular morbidity (most notably myocardial infarction [13] or new or worsening heart failure [14]). Symptomatic patients have worse outcomes.” (pg. 488) Continue reading
Tolstrup MB, Watt SK, Gögenur I. Reduced Rate of Dehiscence After Implementation of a Standardized Fascial Closure Technique in Patients Undergoing Emergency Laparotomy. Ann Surg. 2017 Apr;265(4):821-826.
Full-text for Emory users.
RESULTS: We included 494 patients from 2014 to 2015 and 1079 patients from our historical cohort for comparison. All patients had a midline laparotomy in an emergency setting. The rate of dehiscence was reduced from 6.6% to 3.8%, P = 0.03 comparing year 2009 to 2013 with 2014 to 2015. Factors associated with dehiscence were male gender [hazard ratio (HR) 2.8, 95% confidence interval (95% CI) (1.8-4.4), P < 0.001], performance status ≥3 [HR 2.1, 95% CI (1.2-3.7), P = 0.006], cirrhosis [HR 3.8, 95% CI (1.5-9.5), P = 0.004], and retention sutures [HR 2.8, 95% CI (1.6-4.9), P < 0.000]. The 30-day mortality rate was 18.4% in the standardized group vs 22.4% in 2009 to 2013, P = 0.057 and 90-day mortality 24.2% vs 30.4%, P = 0.008.
CONCLUSION: The standardized procedure of closing the midline laparotomy by using a “small steps” technique of continuous suturing with a slowly absorbable (polydioxanone) suture material reduces the rate of fascial dehiscence.
