
Menahem B, Alves A, Regimbeau JM, Sabbagh C. Colorectal family polyadenomatous diseases. What management in 2020? J Visc Surg. 2020 Apr;157(2):127-135.
Full-text for Emory users.

“The two main genetic conditions responsible for adenomatous polyposis are familial adenomatous polyposis (FAP) (caused by an autosomal dominant mutation of the APC gene) and MUTYH-associated polyposis (MAP) (caused by bi-allelic recessive mutations of the MUTYH (MutY human homolog) gene). FAP is characterized by the presence of >1000 polyps and a young age at diagnosis (mean age of 10). In the absence of screening, the risk of colorectal cancer at age 40 is 100%. It is recommended to start screening at the age of 10-12 years. For patients with FAP and MAP, it is also recommended to screen the upper gastrointestinal tract (stomach and duodenum). In FAP, prophylactic surgery aims to reduce the risk of death without impairment of patient quality of life. The best age for prophylactic surgery is not well-defined; in Europe, prophylactic surgery is usually performed at age 20 as the risk of cancer increases sharply during the third decade. There are three main surgical procedures employed: total colectomy with an ileorectal anastomosis, restorative coloproctectomy with a J pouch anastomosis and coloproctectomy with a stoma. Restorative coloproctectomy with J pouch anastomosis is the reference procedure; however, disease can vary in severity from one patient to another and this must be taken into account to decide which procedure should be performed. In conclusion, the management of adenomatous polyposis is complex but is well-defined by guidelines, particularly in France.”
Augustin T, et al. Tailored surgical treatment of duodenal polyposis in familial adenomatous polyposis syndrome. Surgery. 2018 Mar;163(3):594-599.
Full-text for Emory users.
Results: Of 767 patients in the database, 63 (8.2%) patients underwent operative treatment: 42 (67%) pancreas-sparing duodenectomy, 15 (24%) pancreatoduodenectomy, and 6 (9.5%) segmental duodenal resection; the majority for Spigelman stages III and IV polyposis. Overall 9.6% had adenocarcinoma postoperatively (28.6% in the pancreatoduodenectomy group; P = .01). The proportion of Spigelman stages III and IV with cancer were 9.5% and 6.5%, respectively. Pathologic upgrade to cancer in patients with low grade dysplasia and high-grade dysplasia on preoperative biopsy was 5.7% and 6.7%, respectively (P = .13). At a median follow-up of 16 years, 7.7% needed a second duodenal polypoisis associated with familial adenomatous polyposis-related operation. Progression to high grade dysplasia or cancer in the stomach occurred in 15.4% of patients. Median overall survival and recurrence-free survival was at least 16 years and 15.6 years. No significant group-based differences were noted on follow-up.
Conclusion: The majority of patients with duodenal polypoisis associated with familial adenomatous polyposis can achieve long-term, cancer-free survival with organ-preserving approaches (pancreas-sparing-duodenectomy and segmental-duodenal-resection) with survival not dependent on the type of resection.
Brosens LA, et al. Prevention and management of duodenal polyps in familial adenomatous polyposis. Gut. 2005 Jul;54(7):1034-43.
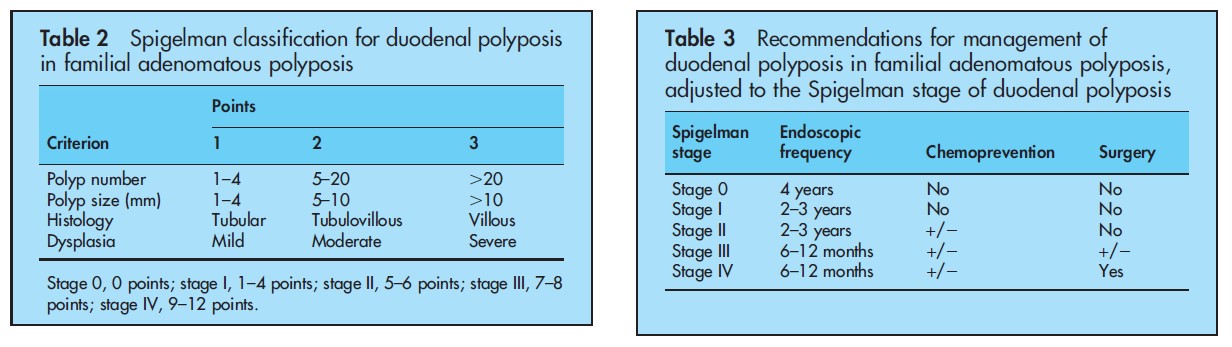
 Figure 4. Spigelman stages of duodenal polyposis. (A) Stage I. (B) Stage II. (C) Stage III. (D) Stage IV.
Figure 4. Spigelman stages of duodenal polyposis. (A) Stage I. (B) Stage II. (C) Stage III. (D) Stage IV.
More PubMed results on duodenal polyposis in FAP.
