
Di Saverio S, et al. Pancreas-sparing, ampulla-preserving duodenectomy for major duodenal (D1-D2) perforations. Br J Surg. 2018 Oct;105(11):1487-1492.
Results: Ten patients were treated with this technique; seven had perforated or bleeding peptic ulcers, two had iatrogenic perforations and one blunt abdominal trauma. Their mean age was 78 (range 65-84) years. Four patients were haemodynamically unstable. The location of the duodenal injury was always D1 and/or D2, above or in close proximity to the ampulla of Vater. The surgical approach was open in nine patients and laparoscopic in one. The mean duration of surgery was 264 (range 170-377) min. All patients were transferred to the ICU after surgery (mean ICU stay 4·4 (range 1-11) days), and the overall mean hospital stay was 17·8 (range 10-32) days. Six patients developed major postoperative complications: cardiorespiratory failure in five and gastrointestinal complications in four. Surgical reoperation was needed in one patient for postoperative necrotizing and bleeding pancreatitis. Two patients died from their complications.

Conclusion: Pancreas-sparing, ampulla-preserving D1-D2 duodenectomy for emergency treatment of major duodenal perforations is feasible and associated with satisfactory outcomes.
Busquets J, et al. Pancreas sparing duodenectomy in the treatment of primary duodenal neoplasms and other situations with duodenal involvement. Hepatobiliary Pancreat Dis Int. 2021 Mar 9:S1499-3872(21)00039-4.
Results: We included 35 patients. Total duodenectomy was performed in 1 patient of adenomatous duodenal polyposis, limited duodenectomy in 7, and third + fourth duodenal portion resection in 27. The indications for scenario 1 were gastrointestinal stromal tumor (n = 13), adenocarcinoma (n = 4), neuroendocrine tumor (n = 3), duodenal adenoma (n = 1), and adenomatous duodenal polyposis (n = 1); scenario 2: retroperitoneal desmoid tumor (n = 2), recurrence of liposarcoma (n = 2), retroperitoneal paraganglioma (n = 1), neuroendocrine tumor in pancreatic uncinate process (n = 1), and duodenal infiltration due to metastatic adenopathies of a germinal tumor with digestive hemorrhage (n = 1); and scenario 3: aortoenteric fistula (n = 3), duodenal trauma (n = 1), erosive duodenitis (n = 1), and biliopancreatic limb ischemia (n = 1). Severe complications (Clavien-Dindo ≥ IIIb) developed in 14% (5/35), and postoperative mortality was 3% (1/35).
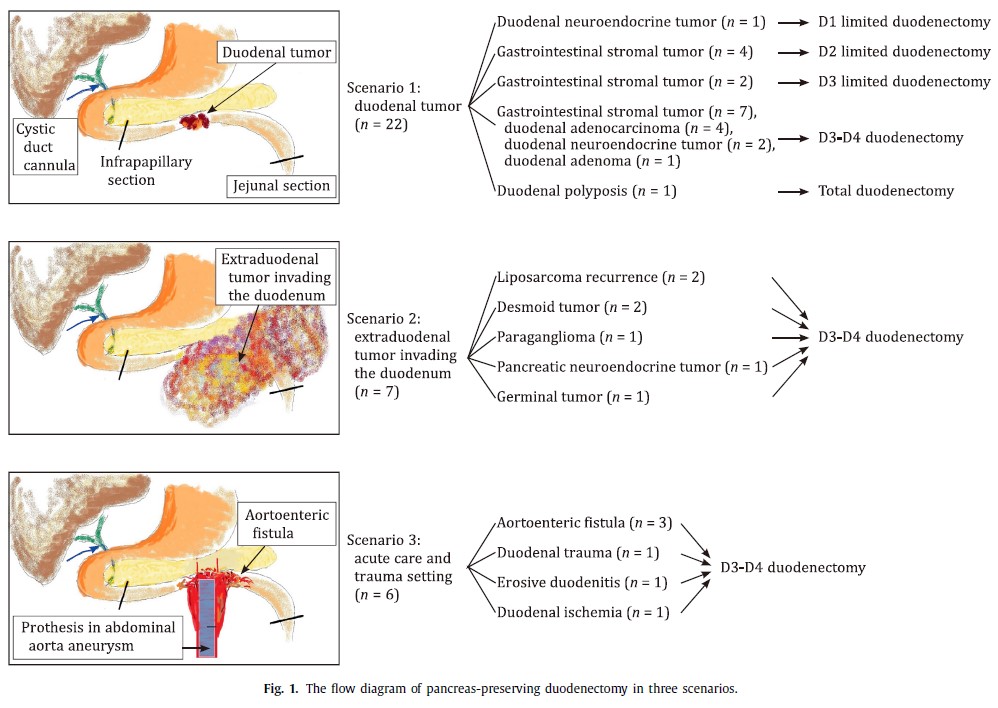
Conclusions: Pancreas-preserving duodenectomy is useful in the management of primary duodenal tumors, and is a technical option for some tumors with duodenal infiltration or in emergency interventions.
More PubMed results on pancreas-preserving duodenectomy.
