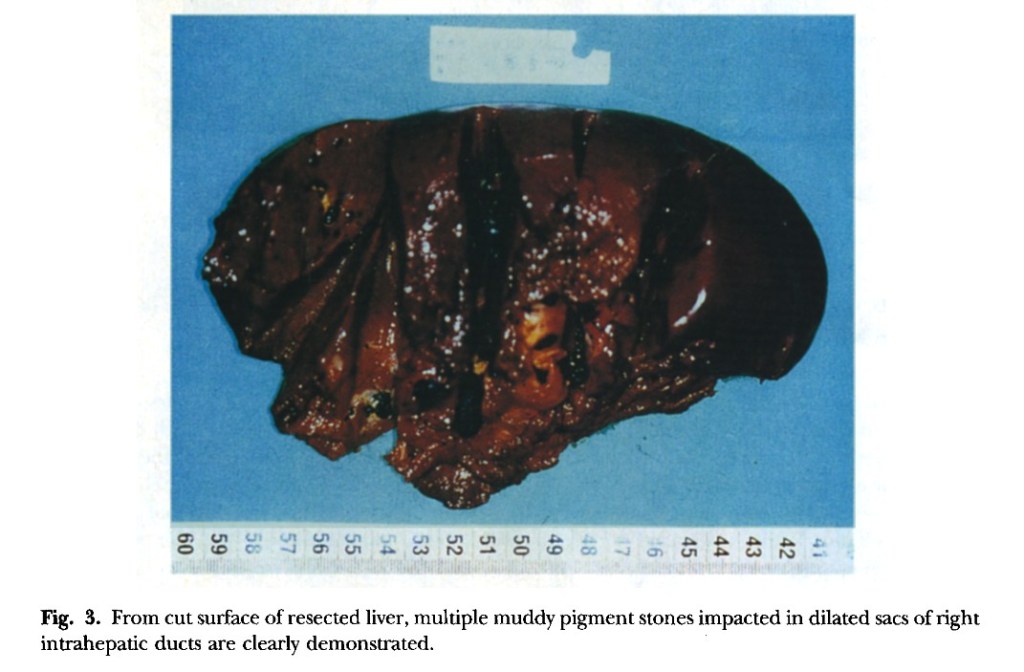
“Hepatic resection has been thought to he the most effective treatment modality for selected patients who have left-sided hepatolithiasis and meet the criteria of resection.” Under the same criteria the role of right hepatic resection, especially right hepatic lobectomy, is still ambiguous for patients who have right-sided hepatolithiasis because of the higher operative risk. This report presents the results of right hepatic lobectomy in the treatment of patients with right-sided hepatolithiasis after careful selection. In particular, we focus on the rationale and indications for this procedure,”
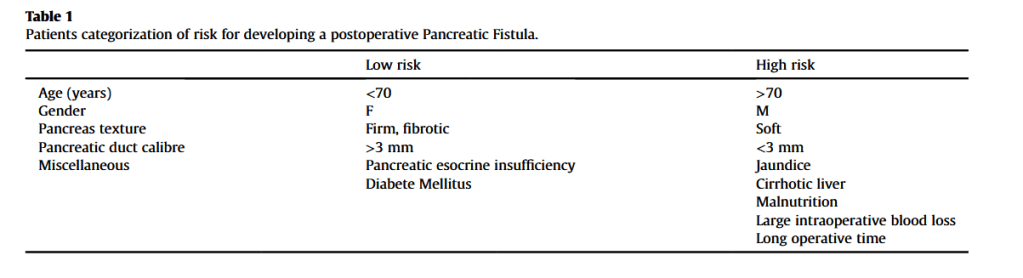
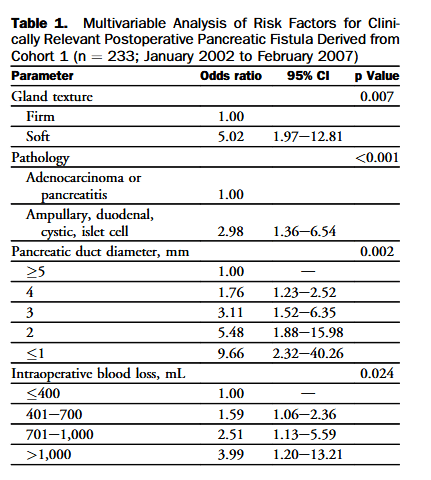
“Pancreaticoduodenectomy (PD) is a complex, high-risk standard surgical procedure that is indicated primarily for periampullary diseases. Central to the entire discipline of PD are postoperative mortality and morbidity. Although operative mortality in patients undergoing PD has decreased, the incidence of postoperative morbidity remains high at 40% to 50%. Postoperative pancreatic fistula (POPF) is the most common complication, with rates ranging from 5% to 30% in previous studies. Many methods have been described to decrease the risk of POPF, including the use of medications (prophylactic octreotide, sealants), prophylactic pancreatic stenting, and improvements in pancreatic reconstruction techniques. The most commonly used pancreatic reconstruction techniques are pancreaticogastrostomy (PG) and pancreaticojejunostomy (PJ).”
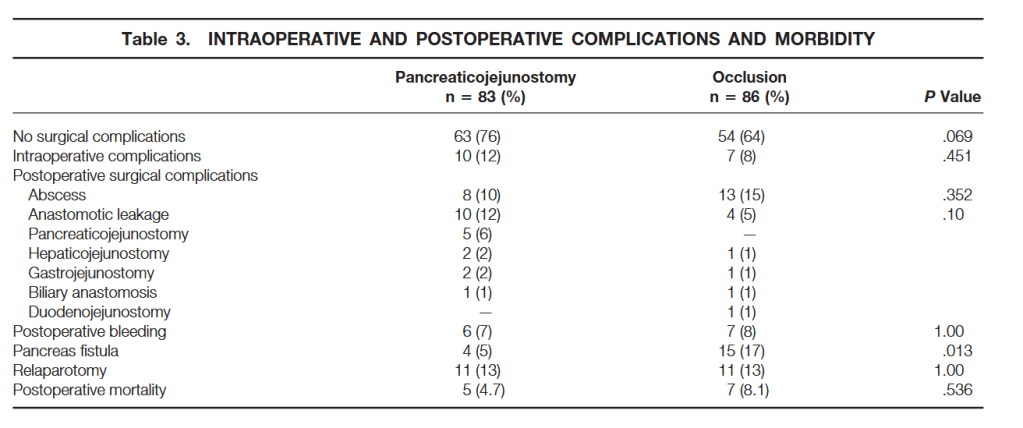
“Pancreatic fistulas and pancreatitis may develop in the pancreatic remnant and may lead to hemorrhage, sepsis, and subsequent death. Procedures to avoid pancreaticojejunostomy were described, including total pancreatectomy. None of these has so far proven to diminish morbidity significantly. Another technique investigated is obliteration closure of the pancreatic duct with a chemical substance, thus avoiding a pancreaticojejunostomy. This method was proposed by Gebhardt et al. They studied the effect of occlusion of the pancreatic duct system with Ethibloc, an alcoholic prolamine, in animal experiments. The pancreatic duct may also be occluded with a fibrin glue solution, Tissucol, which was found to have a more protective effect on beta cell function than the other solutions used.”
“Pancreatoduodenectomy (PD) is the gold standard surgical procedure performed for both benign and malignant diseases of the pancreas and periampullary region. Since the introduction of PD by Whipple in 1941, the treatment of the pancreatic stump was felt as primary issue due to the frequency of the complications. Advances in medical and surgical care have made the mortality rate after PD declined dramatically (0e5%), even in centres with experienced surgeons. However, the morbidity rate remains quite high, approaching the 50%. The most common complications after PD are pancreatic fistula, late gastric empty, haemorrhage, hepatic-jejunostomy leakage, wound infection and intraabdominal abscess, which affect mortality rate, hospitalization and costs. At present, pancreatic fistula (PF) is the most significant complication, with a rate ranges from 5% to 40% even in tertiary centers. About the 40% of the patient deaths are the results of septic and haemorrhagic complication following PF. Although, attempting to reduce complications, many refinements of the cur- rent surgical techniques, pancreatico-jejunostomy, pancreaticogastrostomy and duct occlusion, have been proposed. Nevertheless, the best method to manage the pancreatic stump is still debated.”
“In recent years, indocyanine green (ICG) fluorescence imaging has emerged as an alternative tool to enhance the visualization of biliary structures during LC. ICG is a fluorescent dye that, when injected intravenously, is preferentially taken up by the liver and excreted into the bile ducts. When exposed to near-infrared light, ICG causes the biliary structures, such as the CD, CBD, and CA, to fluoresce, making them more distinguishable from surrounding tissues thereby facilitating real-time visualization of biliary structures during the dissection of Calot’s triangle. The timing of ICG injection is critical to ensure that the biliary anatomy lights up distinctly without interference from non-biliary structures. However, the routine use of ICG fluorescence imaging in LC has not yet been standardized, and there is ongoing debate about whether its widespread adoption would significantly reduce the incidence of BDI and improve patient outcomes. This systematic review aims to provide a comprehensive evaluation of the efficacy and safety of ICG fluorescence imaging in LC, specifically comparing its impact on the incidence of BDI to that of conventional white light (WL) imaging.”
Table 4. Comparison of visualization of biliary structures and incidence of BDI using ICG fluorescence vs WL in LC.
BDI, bile duct injury; CBD, common bile duct; CD, cystic duct; CHD, common hepatic duct; ICG, indocyanine green; LC, laparoscopic cholecystectomy; WL, white light; -, not specified
Author(s) and year
Visualization of CD
Visualization of CBD
Visualization of CHD
Visualization of the CD-CBD junction
Incidence of BDI using ICG
Incidence of BDI using WL
Symeonidis et al., 2024
No significant difference (p = 0.225)
No significant difference (p = 0.276)
No significant difference (p = 0.940)
No significant difference (p = 0.827)
0
0
Ma et al., 2023
Before dissecting Calot’s: no significant difference (p = 0.075). After dissecting Calot’s: ICG signifi-cantly improved visualization (p = 0.02)
Before dissecting Calot’s: no significant difference (p = 0.075). After dissecting Calot’s: ICG signifi-cantly improved visualization (p = 0.02)
–
–
0
0
Xu et al., 2023
–
–
–
–
0
0
Stolz et al., 2023
No significant difference
No significant difference
No significant difference
No significant difference
–
–
Lie et al., 2023
Improved RR 1.24, 95% CI 1.07–1.43, p = 0.003
Improved: RR 1.31, 95% CI 1.07–1.60, p = 0.009
–
–
No significant difference: (RR 0.34, 95% CI 0.07–1.58, p = 0.17)
No significant difference: (RR 0.34, 95% CI 0.07–1.58, p = 0.17)
Losurdo et al., 2022
–
–
–
–
0
1.4%, p = 0.728
Lacuzzo et al., 2022
–
–
–
–
0
0
Jin et al., 2022
–
–
–
–
0
1.83%, p = 0.389
Lim et al., 2021
No significant difference: RR = 0.90, p = 0.12, 95% CI 0.79– 1.03, I² = 74%
No significant difference: RR = 0.82, p = 0.09, 95% CI 0.65– 1.03, I² = 87%
ICG significantly improved visualization: RR = 0.58, p = 0.03, 95% CI 0.35–0.93, I² = 91%
No significant difference: RR = 0.68, p = 0.06, 95% CI 0.45– 1.02, I² = 94%
0
2 (0.55%)
Dip et al., 2021
–
–
–
–
1 (0.06%)
12 (0.25%)
Broderick et al., 2021
–
–
–
–
0
1 (0.1%), p = 1
Keeratibharat, 2021
ICG signifi-cantly improved visualization, p = 0.001
ICG signifi-cantly improved visualization, p = 0.002
ICG signifi-cantly improved visualization, p = 0.000
–
0
0
Ambe et al., 2019
–
–
–
–
0
0
Dip et al., 2019
Before dissecting Calot’s: ICG signifi-cantly improved visualization (p ≤ 0.001). After dissecting Calot’s: no significant difference (p = 0.83)
Before and after dissecting Calot’s: ICG signifi-cantly improved visualization (p < 0.001)
Before and after dissecting Calot’s: ICG signifi-cantly improved visualization (p < 0.001)
Before and after dissecting Calot’s: ICG signifi-cantly improved visualization (p < 0.001)
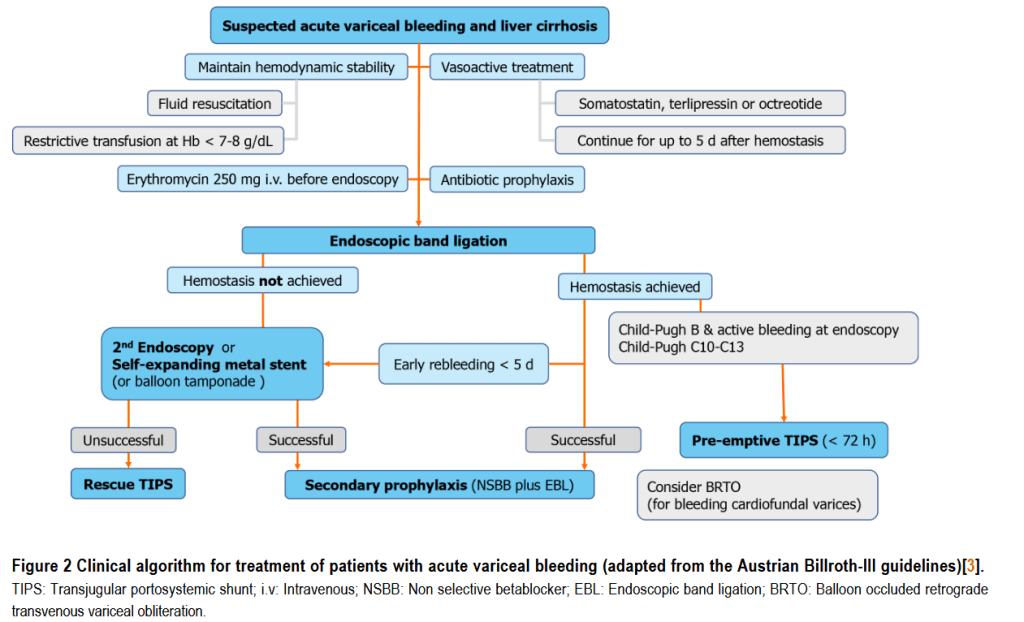
“Variceal bleeding is a severe, and often deadly, complication of portal hypertension. Screening for varices, effective bleeding prophylaxis and standardized management of bleeding is critical to improve clinical outcomes. While carvedilol seems to be the treatment of choice for primary prophylaxis in compensated cirrhosis, the use of hepatic venous pressure gradient measurements and safety of non-selective betablockers in advanced cirrhosis with refractory ascites is controversial. The pre-emptive use of transjugular intrahepatic portosystemic shunt within 72 h after variceal bleeding prevents rebleeding and mortality in Child C10-C13 patients.”
“Despite advancements in operative technique and improvements in postoperative outcomes, pancreatic fistula is widely considered to be the most common and troublesome complication after pancreatic resection. It represents the factor most often linked with postoperative mortality, certain complications such as delayed gastric emptying, longer hospital stays, readmissions, and increased costs. Furthermore, it frequently delays timely delivery of adjuvant therapies, and reduces overall patient survival. Placement of pancreatic duct stents, the use of somatostatin analogs or adhesive sealants, or modifications in reconstruction technique have done little to change the incidence or alter the impact of postoperative pancreatic fistulas (POPF).”