
A discussion this week included a diagnostic CTA prior to flourscopic angiography.
Reference: Wells ML, et al. CT for evaluation of acute gastrointestinal bleeding. RadioGraphics. 2018 Jul-Aug;38(4):1089-1107. doi:10.1148/rg.2018170138
Summary: “Teaching point: CT angiography is gaining popularity for use in emergent evaluations of acute GI bleeding. It has potential for use in the first-line evaluation of acute LGIB and the evaluation of UGIB after failed or nondiagnostic endoscopy.”
An example algorithm for diagnostic evaluation in a patient with acute bleeding in whom UGIB is considered unlikely is provided in Figure 2 below. CT angiography is widely available, and with appropriate triage, an angiogram may be acquired within a few minutes. Shortening the delay prior to evaluation is important, given that even a massive hemorrhage can start and stop rapidly over time and lengthening the time between the start of known bleeding and the subsequent implementation of radiologic evaluation results in fewer positive-result examinations.
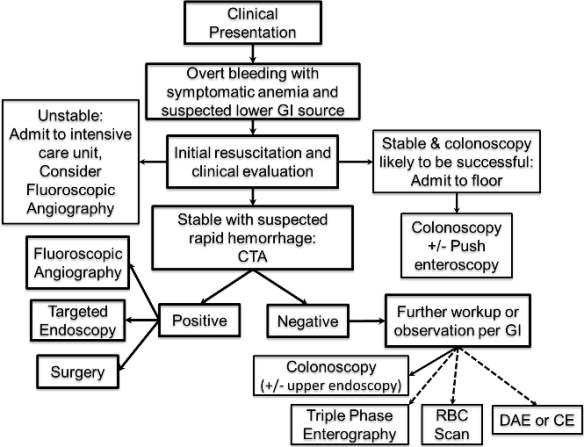
Figure 2. Example of a diagnostic algorithm used to evaluate acute LGIB. CE = capsule endoscopy, CTA = CT angiography, DAE = device-assisted endoscopy.
CT angiography is more sensitive than fluoroscopic angiography for detection of active extravasation, but less sensitive than RBC scanning, being able to depict bleeding at a rate of 0.3–0.5 mL/min. The examination is sensitive for detection of arterial and venous sources of bleeding. In the absence of active bleeding, CT angiography can be performed to detect bowel wall disease such as vascular malformations and masses. However, compared with multiphase CT enterography, it is relatively limited in the assessment of the bowel wall and intraluminal contents.
CT angiographic protocols designed for evaluation of acute GI bleeding are optimized for rapid throughput and maximal sensitivity in detection of active extravasation and bowel wall disease. CT angiography is performed without the administration of oral contrast material. Positive oral contrast material is not administered because it would obscure luminal iodine extravasation and bowel wall enhancement. Neutral oral contrast material is also not administered due to the time delay required for drinking. The possibility of the neutral contrast agent diluting the extravasated iodine and subsequently limiting visibility of the iodine has been suggested but not demonstrated in a published study. Intravenous administration of iodinated contrast material is a required component of CT angiography. The examination may be performed by acquiring images during three phases—non–contrast material–enhanced, arterial, and portal venous phases—or by performing two-phase dual-energy CT during the arterial and portal venous phases.
