
Al Shakarchi J, et al. Surgical techniques for haemodialysis access-induced distal ischaemia. J Vasc Access. 2016 Jan-Feb;17(1):40-6.
 Results: Following strict inclusion/exclusion criteria by two reviewers, twenty-seven studies of surgical interventions were included and divided into subgroups for banding, DRIL, PAI and RUDI procedures. Both DRIL and banding procedures were found to have high rates of symptomatic relief. In addition, the DRIL has a significantly lower rate of early thrombosis than banding although the more recent papers seem to suggest that early thrombosis is less of a problem in banding. PAI and RUDI showed some promise but there were too few studies to be able to make any clear conclusions.
Results: Following strict inclusion/exclusion criteria by two reviewers, twenty-seven studies of surgical interventions were included and divided into subgroups for banding, DRIL, PAI and RUDI procedures. Both DRIL and banding procedures were found to have high rates of symptomatic relief. In addition, the DRIL has a significantly lower rate of early thrombosis than banding although the more recent papers seem to suggest that early thrombosis is less of a problem in banding. PAI and RUDI showed some promise but there were too few studies to be able to make any clear conclusions.
Conclusions: All four procedures have high success rate in relieving ischaemic symptoms with the DRIL procedure having a significantly better vascular access patency rate than other techniques, although further well designed studies are required to compare all four surgical techniques.
Leake AE, et al. Management and outcomes of dialysis access-associated steal syndrome. J Vasc Surg. 2015 Mar;61(3):754-60. Free full-text.
 Click to enlarge image.
Click to enlarge image.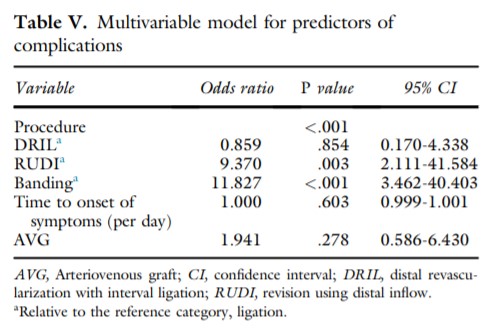
Results: A total of 201 patients had 218 episodes of DASS. Mean age was 65 years, and 62% were women. DASS was caused by 175 arteriovenous fistulas (80%), 41 upper extremity prosthetic grafts (19%), and two thigh grafts (1%); 87% were brachial artery based. A portion (22%) were referred for DASS from outside practices. All patients had grade 2 (48%) or grade 3 (52%) DASS; 92% (185) were available for follow-up, with a median time to first follow-up of 23 days. Surgical procedures included ligation (73), distal revascularization with interval ligation (DRIL) (59), revision using distal inflow (RUDI) (21), banding (38), proximalization of arterial inflow (12), and distal radial artery ligation (13). There were no differences in preoperative comorbidities between treatment groups. The 30-day complications included continued steal, thrombosis, bleeding, infection, and mortality. Ligation and DRIL were performed most often for grade 3 steal. Ligation and banding were performed most acutely (median time to intervention after access creation of 39 and 24 days vs DRIL and RUDI at 97 and 100 days). Fistula preservation was 0% for ligation, 100% for DRIL, 95% for RUDI, and 89% for banding (P < .01). Improvement of symptoms ranged from 75% (banding) to 98% (DRIL) (P = .005). Women were less likely to have DRIL but more likely to have ligation (P = .001). Complications were highest in the banding (49%) and RUDI (37%) groups. Average mortality was 3.5%, with no significant differences among groups. During the study period, 3287 access procedures were performed, and access volume steadily increased (2003-2008, 1312 access creations; 2008-2013, 1975). Percentage of fistulas (79% vs 86%), incidence of steal (4% vs 6%), and percentage of DRILs (25% vs 28%) were consistent across the two study periods.
Mickley V. Steal syndrome–strategies to preserve vascular access and extremity. Nephrol Dial Transplant. 2008 Jan;23(1):19-24. Free full-text.


Created 10/01/20; updated 06/17/22.
