
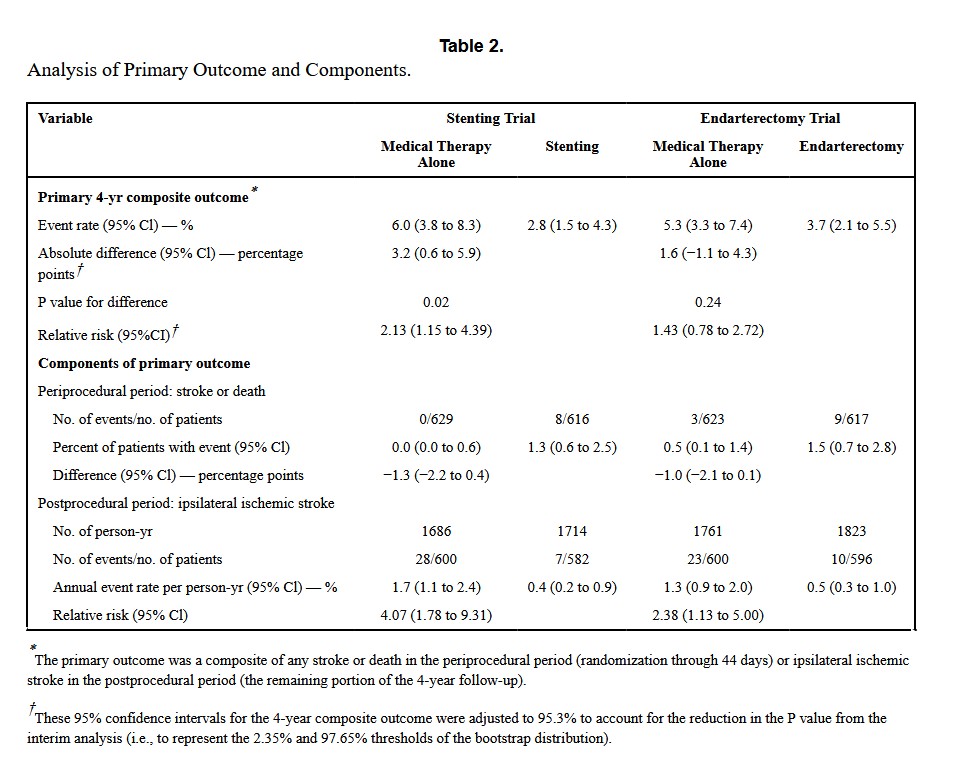
“The treatment of high-grade carotid-artery stenosis varies considerably internationally. Some countries limit revascularization primarily to patients with symptoms, whereas others more commonly recommend that asymptomatic patients undergo revascularization. In the United States, 75 to 80% of patients who undergo carotid-artery stenting or endarterectomy are asymptomatic. Randomized trials from the 1990s and early 2000s showed that carotid
endarterectomy led to a lower risk of stroke among asymptomatic patients with high-grade
stenosis than medical therapy. Improvements in carotid endarterectomy, carotid-artery
stenting, and medical therapy and the results of two recent small trials have challenged
our understanding of appropriate treatments. Here, we present results from the Carotid
Revascularization and Medical Management for Asymptomatic Carotid Stenosis Trials
(CREST-2), which tested whether carotid artery stenting or carotid endarterectomy plus
intensive medical management would be superior to intensive medical management alone
for preventing stroke in patients with high-grade carotid stenosis without recent stroke
symptoms.”


 Results: Following strict inclusion/exclusion criteria by two reviewers, twenty-seven studies of surgical interventions were included and divided into subgroups for banding, DRIL, PAI and RUDI procedures. Both DRIL and banding procedures were found to have high rates of symptomatic relief. In addition, the DRIL has a significantly lower rate of early thrombosis than banding although the more recent papers seem to suggest that early thrombosis is less of a problem in banding. PAI and RUDI showed some promise but there were too few studies to be able to make any clear conclusions.
Results: Following strict inclusion/exclusion criteria by two reviewers, twenty-seven studies of surgical interventions were included and divided into subgroups for banding, DRIL, PAI and RUDI procedures. Both DRIL and banding procedures were found to have high rates of symptomatic relief. In addition, the DRIL has a significantly lower rate of early thrombosis than banding although the more recent papers seem to suggest that early thrombosis is less of a problem in banding. PAI and RUDI showed some promise but there were too few studies to be able to make any clear conclusions.