
One discussion this week included nodal management after neoadjuvant chemotherapy (NAC).
Reference: Pilewskie M and Morrow M. Axillary nodal management following neoadjuvant chemotherapy. JAMA Oncology. 2017 Apr 1;3(4):549-555.
Summary: The increasing use of NAC has raised questions about the optimal approach to the axilla, including accuracy and timing of sentinel lymph node biopsy (SLNB) in patients who are clinically node negative (cN0) at presentation, use of NAC to avoid axillary lymph node dissection (ALND) in patients presenting with node-positive disease, and the relative importance of pre-and post-NAC stage in predicting the risk of locoregional recurrence (LRR).
The decrease in nodal metastases in cN0 patients undergoing post-NAC axillary staging and the increasing rates of pCR in the breast in patients treated with current chemotherapy regimens led to the study of SLNB among patients presenting with cN+ disease. Table 3 (below) summarizes data from three prospective, multi-institutional trials assessing the accuracy of SLNB after NAC among node-positive patients.
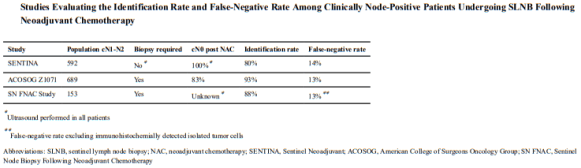
The authors conclude: NAC reduces the need for ALND, and SLNB is an accurate
method of determining nodal status post NAC. The demonstration that SLNB accurately stages the axilla after NAC regardless of the presenting nodal stage (cN0, cN1) provides an important rationale for the use of NAC for axillary downstaging in patients who are candidates for breast-conserving surgery at presentation or who desire mastectomy. SLN identification rates and FNRs in those who are cN0 are similar to those seen with initial SLN surgery, and nodal recurrence after a negative SLNB is uncommon.
Additional Reading: Boughey JC, et al. Sentinel lymph node surgery after neoadjuvant chemotherapy in patients with node-positive breast cancer: the ACOSOG Z1071 (Alliance) clinical trial. JAMA. 2013 Oct 9;310(14):1455-1461. doi:10.1001/jama.2013.278932.
