
Barrionuevo P, Malas MB, Nejim B, et al. A systematic review and meta-analysis of the management of visceral artery aneurysms. J Vasc Surg. 2019;70(5):1694–1699.
Full-text for Emory users.
“We included 33 case series of 523 splenic artery aneurysms treated with an endovascular approach and 22 series of 252 splenic artery aneurysms treated with open surgery. Short-term and long-term mortality rates were very low and not significantly different between the two interventions. Mortality was high for ruptured aneurysms treated with an open approach, with an event rate of 0.29 (95% CI, 0.04-0.71). End-organ infarction and gastrointestinal complications rates were not significantly different between the two approaches. The need for reintervention was lower for open surgery 0.00 (95% CI, 0.00-0.11) than for the endovascular approach 0.07 (95% CI, 0.01-0.17). The risk of access site complications for the endovascular approach was low at 0.02 (95% CI, 0.00-0.09). Rates of PES and coil migration were 0.38 (95% CI, 0.04-0.79) and 0.08 (95% CI, 0.00-0.24), respectively. Data were insufficient to identify a difference in mortality based on aneurysm size.”
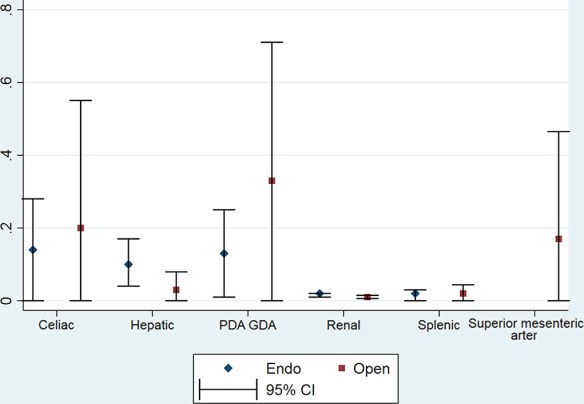
Fig 2. Mortality rates for open and endovascular (Endo) approaches according to aneurysm location. CI, Confidence interval; GDA, gastroduodenal artery; PDA, pancreaticoduodenal artery.
Sticco A, Aggarwal A, Shapiro M, et al. A comparison of open and endovascular treatment strategies for the management of splenic artery aneurysms. Vascular. 2016;24(5):487–491.
Emory users, you can request the full-text article via ILL here.
“Splenic artery aneurysms are rare with an incidence of less than 0.8%. Evidence to support an endovascular management strategy over open surgical repair for SAA is limited. We used the Nationwide Inpatient Sample to compare open to endovascular SAA repair by assessing postoperative outcomes, length of hospital stay, and mortality. Multivariate logistic regression analysis was done to determine predictors of postoperative complications. There were 2316 admissions with a diagnosis code for SAA [347 (14.9%) endovascular repair and 112 (4.8%) open surgery]. There was a statistically significant lower rate of cardiac (2.3% vs 6.9%, P = 0.05) and pulmonary (8.9% vs 16.1%, P = 0.05) complications for the endovascular repair group. The risk of surgical site infection was also lower (0.6% vs 5.1%, P = 0.01) in the endovascular group. Median in-hospital LOS was greater for open repairs (6 vs. 4 days, P = 0.01). There were no statistically significant differences across procedures for renal complications (8.9%, P = 0.88) or in-hospital mortality (3%, P = 0.99). Regression analysis established procedure type to be independent predictor of postoperative complications. Endovascular repair of SAA is therefore associated with a lower complication rate and less resource utilization but no difference in mortality peri-operatively. This may justify an endovascular first treatment strategy in the management of SAA.”
Mohan IV, Stephen MS. Peripheral arterial aneurysms: open or endovascular surgery?. Prog Cardiovasc Dis. 2013;56(1):36–56.
Full-text for Emory users.
“Laparoscopic splenectomy may be considered to be a safe therapeutic option for SAA patients with a lower risk than conventional open surgery. [111] In one of the largest series of endovascular intervention for SAA, technical success was achieved in 96%, and no conversions or mortality. 35% of cases had post-embolization syndrome, mostly related to distal splenic intervention, and 6% required reintervention. Ten percent had left upper quadrant pain and all others were asymptomatic. Postembolization syndrome is characterized by a combination of fevers, abdominal pain, ileus, and pancreatic inflammation. This syndrome is observed in 30% to 80% of patients, but usually resolves within 4 to 5 days. [109, 112] The authors concluded that endovascular ablation remains a durable, effective treatment for SAA. [112] Endovascular intervention success rates of approximately 85% from endovascular intervention are lower than direct surgical intervention, although associated operative morbidity and mortality rates are significantly reduced. [103, 111, 112, 113]” (Mohan, 2013, p. 45)
Recommendation: “We recommend an endovascular first approach, especially in patients with pseudoaneurysms. Open surgical intervention is still the treatment of choice in cases of aneurysm rupture and haemodynamic instability, and those with unfavourable anatomy for the endovascular option. The laparoscopic approach may offer an advantage to conventional laparotomy.” (Mohan, 2013, p. 46)
More PubMed results on the management of SAAs.
