
Razavi MK, Razavi MD. Stent-graft treatment of mycotic aneurysms: a review of the current literature. J Vasc Interv Radiol. 2008;19(6 Suppl):S51–S56.
Full-text for Emory users.
“Mycotic aneurysms are rare but are associated with a high risk of rupture if not treated promptly. The early mortality rate associated with traditional surgery depends on patients’ condition and can be as high as 43%. The use of stent-grafts is less invasive but the outcome is unproven in the setting of infected aneurysms. In an attempt to better elucidate the role of stent-grafts in this setting, a literature search was performed to examine 52 articles describing 91 patients with mycotic aneurysms who were treated with stent-grafts. The early mortality rate was 5.6%. Incidences of late aneurysm-related mortality and complications were 12.2% and 7.8%, respectively. The most consistent predictor of poor outcome was development of aortoenteric fistula. Although the 30-day mortality rate associated with the use of stent-grafts appears to be lower than that associated with surgery, late aneurysm-related events are frequent and warrant a more vigilant follow-up regimen than used with noninfected aneurysms.”
Table 2. Location of Mycotic Aneurysms Treated with Stent-Grafts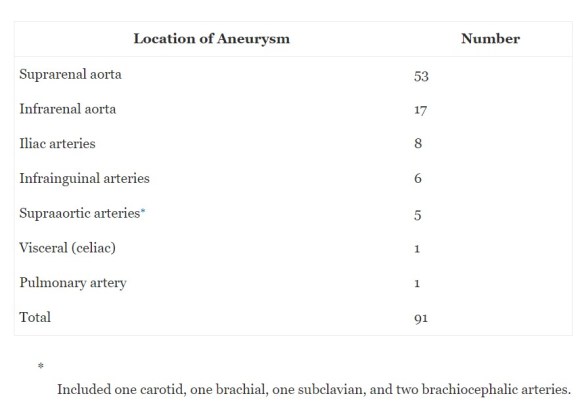
Table 3. Current Literature Review of Endovascular Therapy of Mycotic Aneurysms
Nakajima K, Kato N, Hashimoto T, et al. Treatment of Infected Aneurysm with Combined Endovascular Aneurysm Repair and Abscess Drainage. J Vasc Interv Radiol. 2018;29(2): 188–193.
Full-text for Emory users.
“Endovascular repair is emerging as a promising alternative since Semba et al. [3] first reported their experience of stent-graft repair for the treatment of mycotic thoracic aortic aneurysms. Endovascular repair has several advantages over open surgical repair such as lack of a need for a large incision or aortic cross-clamping. Since the first report, several case series of endovascular repair have been reported, supporting the efficacy of the procedure. [4, 9, 10] Indeed, EVAR was the only choice of treatment in one of our cases with a hostile abdomen and a ruptured aneurysm. Moreover, EVAR was deemed a better choice in another case wherein the aneurysm was located at the suprarenal aorta, which is reported to be a predictive factor of aneurysm-related mortality. [2, 10, 11] The 1-year survival rate was 91% in the latest and the largest series, being superior to that of open surgical repair. [12] The 5-year survival rate was 55% in the series, which is comparable with that of patients with a noninfected aneurysm treated with EVAR. [13]
However, there remains an important issue with this treatment strategy: placement of a foreign body including stent grafts and coils in an infected field may lead to persistent infection or delayed rupture. Indeed, in previous reports, infection-related complications were observed in 22–27% of cases treated with EVAR, and the mortality rate of those patients exceeded 70%. [4, 10, 12] Although complete removal of the infected tissue including the aorta or artery, lavage of the explored field, and embedding of the omentum are possible during open surgical repair, these are not possible in EVAR. Therefore, some authors insist that EVAR should be regarded as a temporary bridge to delayed open repair. [14, 15]” (Chino, 2016, pgs. 289.e13-e14)
More PubMed results on management of MAs.
