
Andreassen M, Ilett E, Wiese D, et al. Surgical Management, Preoperative Tumor Localization, and Histopathology of 80 Patients Operated on for Insulinoma. J Clin Endocrinol Metab. 2019 Dec 1;104(12):6129-6138.
Full-text for Emory users.
Results: Eighty patients were included. Seven had a malignant tumor. A total of 312 diagnostic examinations were performed: endoscopic ultrasonography (EUS; n = 59; sensitivity, 70%), MRI (n = 33; sensitivity, 58%), CT (n = 55; sensitivity, 47%), transabdominal ultrasonography (US; n = 45; sensitivity, 40%), somatostatin receptor imaging (n = 17; sensitivity, 29%), 18F-fluorodeoxyglucose positron emission tomography/CT (n = 1; negative), percutaneous transhepatic venous sampling (n = 10; sensitivity, 90%), arterial stimulation venous sampling (n = 20; sensitivity, 65%), and intraoperative US (n = 72; sensitivity, 89%). Fourteen tumors could not be visualized. Invasive methods were used in 7 of these 14 patients and localized the tumor in all cases. Median tumor size was 15 mm (range, 7 to 80 mm). Tumors with malignant vs benign behavior showed less staining for insulin (3 of 7 vs 66 of 73; P = 0.015) and for proinsulin (3 of 6 vs 58 of 59; P < 0.001). Staining for glucagon was seen in 2 of 6 malignant tumors and in no benign tumors (P < 0.001). Forty-three insulinomas stained negative for somatostatin receptor subtype 2a.
Conclusion: Localization of insulinomas requires many different diagnostic procedures. Most tumors can be localized by conventional imaging, including EUS. For nonvisible tumors, invasive methods may be a useful diagnostic tool. Malignant tumors showed reduced staining for insulin and proinsulin and increased staining for glucagon.
Wei J, et al. Diagnosis and surgical management of insulinomas in 33 consecutive patients at a single institution. Langenbecks Arch Surg. 2016 Nov;401(7):1019-1025.
Full-text for Emory users.
 Click to enlarge.
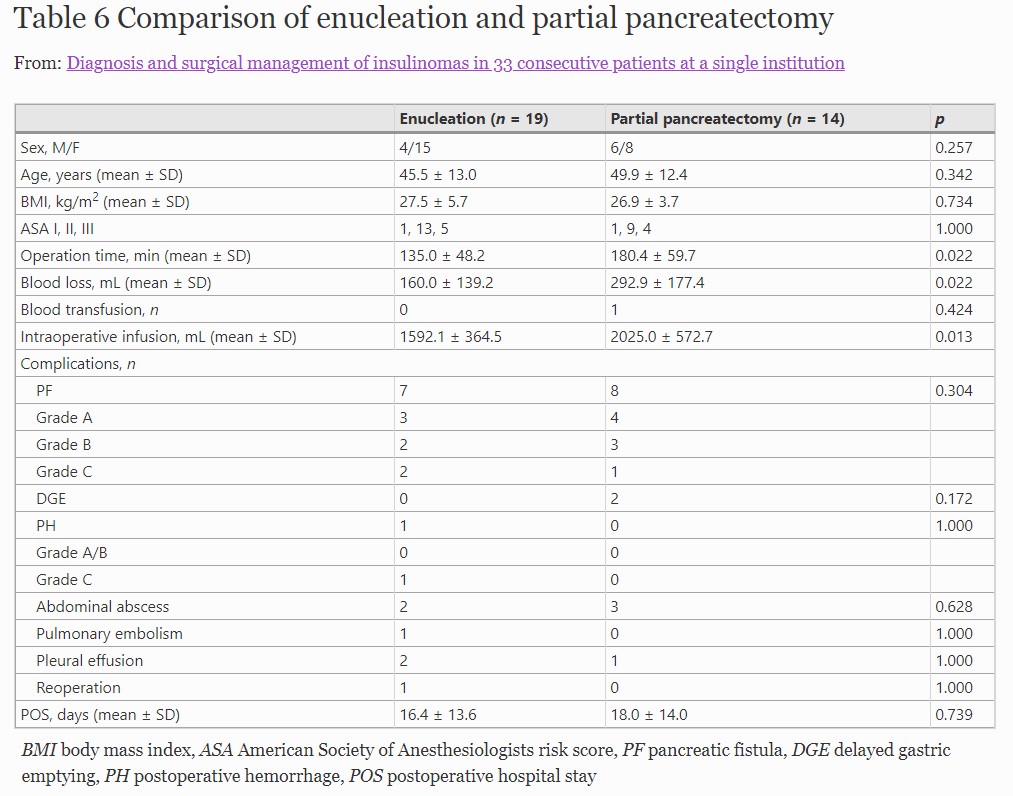
Click to enlarge.Results: The median time from the first onset of symptoms to diagnosis was 24 months (range 3 days to 50 years). All cases presented with Whipple’s triad and had a fasting insulin to glucose ratio higher than 0.33. The preoperative detection rates of transabdominal ultrasonography, CT, MRI, and EUS were 22 % (2/9), 72 % (23/32), 75 % (9/12), and 80 % (4/5), respectively. Intraoperative manual palpation localized all cases. Enucleation was performed in 58 % of cases (19/33), partial pancreatic resection in 39 % (13/33), and enucleation plus partial resection in 3 % (1/33). Pancreatic fistula was the most common complication and occurred in 15 patients (45 %), including seven grade A, five grade B, and three grade C fistulas. There was no mortality. When compared with partial pancreatectomy, enucleation held a significant advantage in operative time and operative bleeding, with no significant differences in demographic data and postoperative complications. During a median follow-up period of 32 months, two patients were lost to follow-up and the remaining 31 patients were without evidence of recurrence.
Conclusions: A fasting insulin release index larger than 0.3 is a reliable indicator for the diagnosis of insulinoma. Intraoperative palpation by an experienced surgeon can effectively complement an uncertain preoperative localization. Compared with partial pancreatic resection, enucleation showed significant benefit in terms of intraoperative blood loss and operation time.
Okabayashi T, et al. Diagnosis and management of insulinoma. World J Gastroenterol. 2013 Feb 14;19(6) :829-37.
“Insulinomas, the most common cause of hypoglycemia related to endogenous hyperinsulinism, occur in 1-4 people per million of the general population. Common autonomic symptoms of insulinoma include diaphroresis, tremor, and palpitations, whereas neuroglycopenenic symptoms include confusion, behavioural changes, personality changes, visual disturbances, seizure, and coma. Diagnosis of suspected cases is based on standard endocrine tests, especially the prolonged fasting test. Non-invasive imaging procedures, such as computed tomography and magnetic resonance imaging, are used when a diagnosis of insulinoma has been made to localize the source of pathological insulin secretion. Invasive modalities, such as endoscopic ultrasonography and arterial stimulation venous sampling, are highly accurate in the preoperative localization of insulinomas and have frequently been shown to be superior to non-invasive localization techniques. The range of techniques available for the localization of insulinomas means that blind resection can be avoided. Intraoperative manual palpation of the pancreas by an experienced surgeon and intraoperative ultrasonography are both sensitive methods with which to finalize the location of insulinomas. A high proportion of patients with insulinomas can be cured with surgery. In patients with malignant insulinomas, an aggressive medical approach, including extended pancreatic resection, liver resection, liver transplantation, chemoembolization, or radiofrequency ablation, is recommended to improve both survival and quality of life. In patients with unresectable or uncontrollable insulinomas, such as malignant insulinoma of the pancreas, several techniques should be considered, including administration of ocreotide and/or continuous glucose monitoring, to prevent hypoglycemic episodes and to improve quality of life.”
