
Zasowski EJ, et al. Identification of Vancomycin Exposure-Toxicity Thresholds in Hospitalized Patients Receiving Intravenous Vancomycin. Antimicrob Agents Chemother. 2017 Dec 21;62(1):e01684-17.
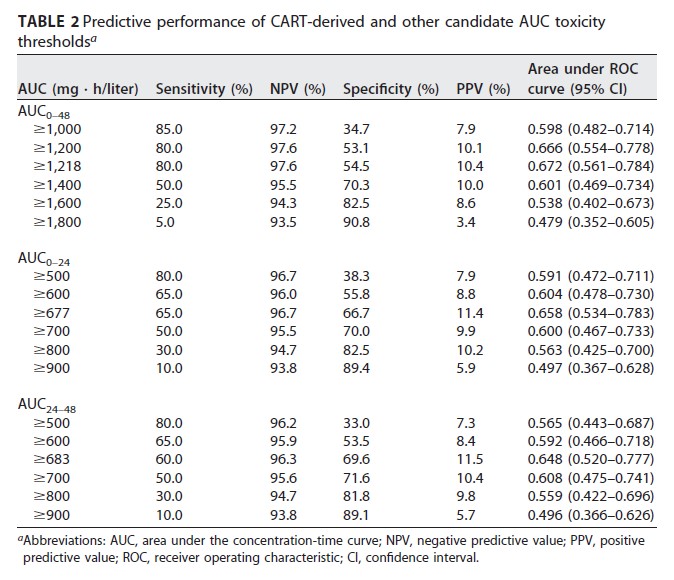
Evidence supports vancomycin therapeutic-drug monitoring by area under the concentration-time curve (AUC), but data to establish an AUC upper limit are limited and published nephrotoxicity thresholds range widely. The objective of this analysis was to examine the association between initial vancomycin AUC and nephrotoxicity. This was a multicenter, retrospective cohort study of adult patients receiving intravenous vancomycin from 2014 to 2015. Nephrotoxicity was defined as a serum creatinine increase of 0.5 mg/liter and 50% from baseline on consecutive measurements. Vancomycin exposure profile during the initial 48 h of therapy was estimated using maximum a posteriori probability Bayesian estimation. Vancomycin AUC and minimum-concentration (Cmin) thresholds most strongly associated with nephrotoxicity were identified via classification and regression tree (CART) analysis. Predictive performances of CART-derived and other candidate AUC thresholds was assessed through positive and negative predictive value and receiver operating characteristic curves. Poisson regression was used to quantify the association between exposure thresholds and nephrotoxicity while adjusting for confounders. Among 323 patients included, nephrotoxicity was significantly higher in patients with AUCs from 0 to 48 h (AUC0-48) of ≥1,218 mg · h/liter, AUC0-24 of ≥677 mg · h/liter, AUC24-48 of ≥683 mg · h/liter, and day 1 Cmin (Cmin24) of ≥18.8 mg/liter. Vancomycin exposure in excess of these thresholds was associated with a 3- to 4-fold-increased risk of nephrotoxicity in Poisson regression. The predictive performance of AUC for nephrotoxicity was maximized at daily AUC values between 600 and 800 mg · h/liter. Although these data support an AUC range for vancomycin-associated nephrotoxity rather than a single threshold, available evidence suggests that a daily AUC limit of 700 mg · h/liter is reasonable.
Hanrahan TP, et al. Factors associated with vancomycin nephrotoxicity in the critically ill. Anaesth Intensive Care. 2015 Sep;43(5):594-9.
Full-text for Emory users.
Abstract: Vancomycin is a glycopeptide antibiotic commonly used in the management of methicillin-resistant Staphylococcus aureus infection. The recent increase in prevalence of methicillin-resistant Staphylococcus aureus with reduced susceptibility to vancomycin has prompted experts to advocate for higher target trough serum concentrations. This study aimed to evaluate the potential consequences of more aggressive vancomycin therapy, by examining the association between higher serum concentrations and acute kidney injury (AKI) in a population of critically ill patients. We collected data for all patients who received vancomycin over a five-year period and evaluated the prevalence of new-onset AKI using the Risk, Injury, Failure, Loss and End-stage (RIFLE) kidney disease criteria. One-hundred and fifty-nine patients provided complete data, with 8.8% manifesting new onset AKI while receiving vancomycin. The median age was 57 (44 to 68) years, while the median trough serum concentration was 16 (10 to 19) mg/l. Multivariate logistic regression analysis identified mean trough concentration (OR=1.174, P=0.024), APACHE II score (OR=1.141, P=0.012) and simultaneous aminoglycoside prescription (OR=18.896, P=0.002) as significant predictors of AKI. These data suggest higher trough vancomycin serum concentrations are associated with greater odds of AKI in the critically ill.
Selby AR, Hall RG 2nd. Utilizing the Patient Care Process to Minimize the Risk of Vancomycin-Associated Nephrotoxicity. J Clin Med. 2019 Jun 1;8(6):781.

More PubMed results on vancomycin dosing, monitoring, and nephrotoxicity.
