
Katsargyris A, et al. Comparison of outcomes with open, fenestrated, and chimney graft repair of juxtarenal aneurysms: are we ready for a paradigm shift? J Endovasc Ther. 2013 Apr;20(2):159-69.
Full-text for Emory users.
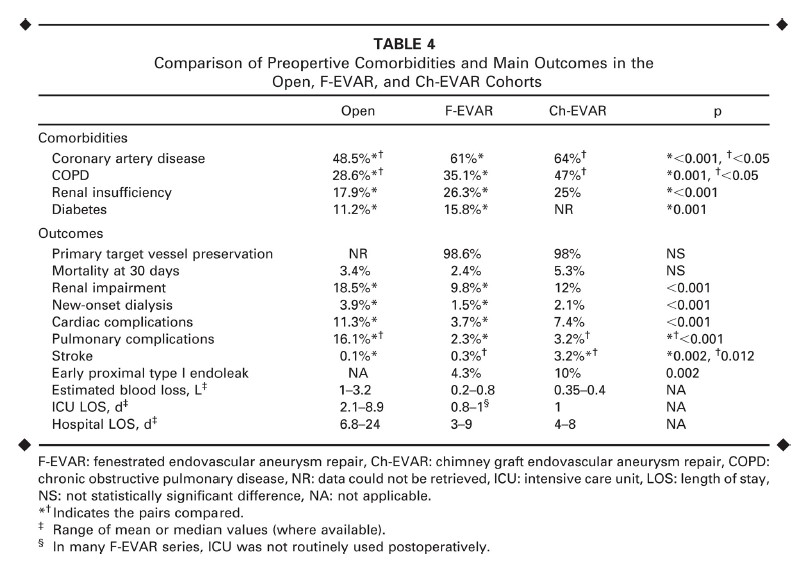
Results: A total of 2465 vessels were targeted with fenestrations and 151 with chimney grafts (CG); intraoperative target vessel preservation was 98.6% and 98.0%, respectively. Cumulative 30-day mortality was 3.4%, 2.4%, and 5.3% for open surgery, F-EVAR and Ch-EVAR, respectively (p=NS). Impaired renal function was noted in 18.5%, 9.8%, and 12% following open surgery, F-EVAR, and Ch-EVAR, respectively (open vs. F-EVAR: p<0.001). New-onset dialysis was required postoperatively in 3.9%, 1.5%, and 2.1%, respectively (open vs. F-EVAR: p<0.001). Postoperative cardiac complications were noted in 11.3%, 3.7%, and 7.4%, respectively (open vs. F-EVAR: p<0.001). The incidence of ischemic stroke was 0.1% and 0.3% following open surgery and F-EVAR, but 3.2% after Ch-EVAR (open vs. Ch-EVAR: p=0.002; F-EVAR vs. Ch-EVAR: p=0.012). Early proximal type I endoleak was lower after F-EVAR compared to Ch-EVAR (4.3% vs. 10%, respectively, p=0.002).
Conclusion: Open surgery remains a safe and effective treatment option for good risk patients with JAA. F-EVAR is associated with low operative mortality, compares favorably to open surgery in terms of morbidity, and current midterm data indicate that it can be a valid treatment option in both low- and high-risk patients. Early results of Ch-EVAR demonstrate feasibility only. In view of the limited number of reports and the lack of long-term data, the technique should be considered only in acute poor surgical risk patients, as a bailout in case of unintentional renal artery coverage, or in elective poor surgical cases that are not suitable for F-EVAR.
