
Dageforde LA, Lillemoe KD. (2020). Management of Acute Cholangitis. In: Cameron JL, Cameron AM (Eds), Current Surgical Therapy, 13th ed. Elsevier: Philadelphia.
“Recent literature advocates for primary closure of the common bile duct after elective CBDE because of complications from T-tube placement. But in patients with cholangitis, placement of a T-tube is necessary for biliary decompression and allows easy access for future cholangiogram if the obstruction does not resolve. T-tube drainage has been associated with bile leak and requires externalization of the tube for several days until postoperative cholangiography demonstrates resolution of obstruction. Primary closure can lead to stricture and bile leak and result in no direct access to the biliary tree for future investigations.”

Fig. 2. Insertion of a T-tube in the common bile duct with subsequent closure using absorbable monofilament suture (4-0 or 5-0). The T-tube is prepared in one of the ways shown. From: Zollinger RM, Jr, Zollinger RM. Atlas of Surgical Operations. 7th ed. New York: McGraw-Hill; 1993.
Lee MJ. (2014). Biliary Intervention. In: Kaufman JA. (Ed.) Vascular and Interventional Radiology: The Requisites. Elsevier: Philadelphia.
“If the patient has a postoperative T-tube in place, then ERCP is inappropriate because any retained stones can be removed easily through the percutaneous tract (Fig. 20-27). If stone removal through the T-tube tract is planned, the T-tube is left in situ for 4-6 weeks until a mature tract develops. Patients return to the hospital for stone removal and are given standard antibiotic prophylaxis. A T-tube cholangiogram is performed to confirm that the stones are still present. In many instances, the stones may have passed in the interval. If a stone is not present, the T-tube can be removed.”

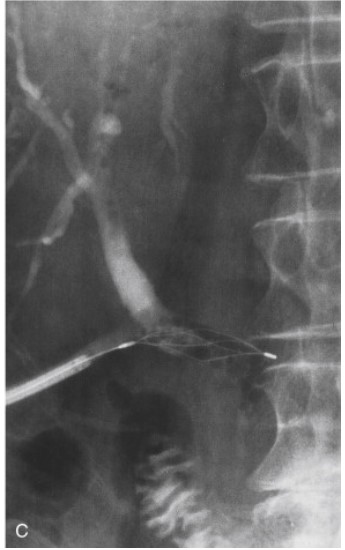
Figure 20-27. Percutaneous extraction of a retained common bile duct stone through a T-tube track. A, The T-tube has been removed and a steerable Burhenne catheter placed through the percutaneous track into the bile duct to the level of the stone (small arrow) . A basket (curved arrow) has been placed distal to the stone. B, The basket is pulled back and manipulated so that the stone (arrow) is engaged within the basket and the basket is then pulled back against the end of the Burhenne catheter. Basket, stone, and Burhenne catheter are then removed through the percutaneous track. C, There is some air present in the lower bile duct. The basket was traversed through the lower bile duct but no further stones were present. Contrast injection at the end of the procedure showed a clear bile duct.
A collection of PubMed citations on T-Tube drainage.
