
Mirrielees JA, et al. Pancreatic Fistula and Delayed Gastric Emptying Are the Highest-Impact Complications After Whipple. J Surg Res. 2020 Jun;250:80-87.
Full-text for Emory users.
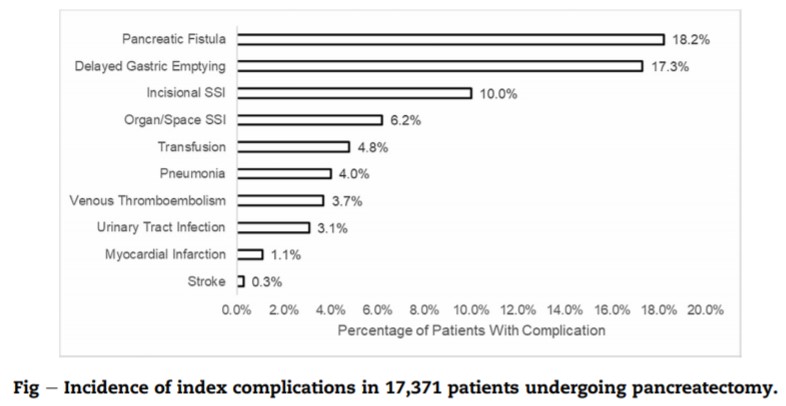
Results: About 10,922 patients undergoing pancreaticoduodenectomy were included for analysis. The most common postoperative complications were DGE (17.3%), POPF (10.1%), incisional SSI (10.0%), and organ/space SSI (6.2%). POPF and DGE were the only complications that demonstrated sizable effects for all clinical and resource utilization outcomes studied. Other complications had sizable effects for only a few of the outcomes or had small effects for all the outcomes.
Ramanathan R, et al. Predictors of Short-Term Readmission After Pancreaticoduodenectomy. J Gastrointest Surg. 2018 Jun;22(6):998-1006.
Full-text for Emory users.
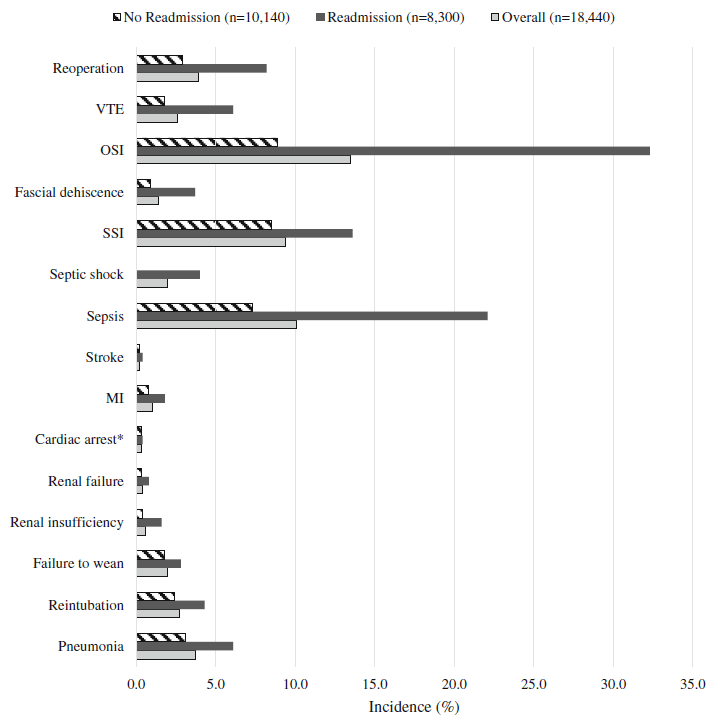
Results: Outcomes of 18,440 pancreaticoduodenectomies were analyzed, and found to have an 18.7% overall readmission rate. Multivariable modeling with pancreatectomy-specific variables increased the predictive value of the model (area under receiver operator characteristic 0.66 to 0.73). Statistically significant independent contributors to readmission included renal insufficiency, sepsis, septic shock, organ space infection, dehiscence, venous thromboembolism, pancreatic fistula, delayed gastric emptying, need for percutaneous drainage, and reoperation.
Conclusions: Large registry analyses of pancreatectomy outcomes are markedly improved by the incorporation of granular procedure-specific data. These data emphasize the need for prevention and careful management of perioperative infectious complications, fluid management, thromboprophylaxis, and pancreatic fistulae.
Qiu J, Li M, Du C. Antecolic reconstruction is associated with a lower incidence of delayed gastric emptying compared to retrocolic technique after Whipple or pylorus-preserving pancreaticoduodenectomy. Medicine (Baltimore). 2019 Aug;98(34):e16663.
Results: Fifteen studies involving 2270 patients were included for final pooled analysis. The overall incidence of DGE was 27.2%. Meta-analysis results showed AC group had lower incidence of DGE (odds ratio, 0.29; 95% confidence interval [CI], 0.16-0.52, P < .0001) and shorter hospital length of stay (weight mean difference, -3.29; 95% CI, -5.2 to -1.39, P = .0007). Days until to liquid and solid diet in the AC group were also significantly earlier than that in the RC group (P = .0006 and P < .0001). There was no difference in operative time, incidence of pancreatic fistula and bile leakage, and mortality, respectively.
Conclusions: AC route of GJ after PD or DJ after PPPD is associated with a lower incidence of DGE. However, the preferred route for GJ or DJ reconstruction remains to be investigated in well-powered, randomized, controlled trial.
Glowka TR, et al. Delayed gastric emptying following pancreatoduodenectomy with alimentary reconstruction according to Roux-en-Y or Billroth-II. BMC Surg. 2017 Mar 20;17(1):24.
Background: Delayed gastric emptying (DGE) remains the most frequent complication following pancreatoduodenectomy (PD) with published incidences as high as 61%. The present study investigates the impact of bowel reconstruction techniques on DGE following classic PD (Whipple-Kausch procedure) with pancreatogastrostomy (PG).
Methods: We included 168 consecutive patients who underwent PD with PG with either Billroth II type (BII, n = 78) or Roux-en-Y type reconstruction (ReY, n = 90) between 2004 and 2015. Excluded were patients with conventional single loop reconstruction after pylorus preserving procedures. DGE was classified according to the 2007 International Study Group of Pancreatic Surgery definition. Patients were analyzed regarding severity of DGE, morbidity and mortality, length of hospital stay and demographic factors.
Results: No difference was observed between BII and ReY regarding frequency of DGE. Overall rate for clinically relevant DGE was 30% (ReY) and 26% (BII). BII and ReY did not differ in terms of demographics, morbidity or mortality. DGE significantly prolongs ICU (four vs. two days) and hospital stay (20.5 vs. 14.5 days). Risk factors for DGE development are advanced age, retrocolic reconstruction, postoperative hemorrhage and major complications.
Conclusions: The occurrence of DGE can not be influenced by the type of alimentary reconstruction (ReY vs. BII) following classic PD with PG. Old age and major complications could be identified as important risk factors in multivariate analysis.
More articles on postoperative complications after pancreatoduodenectomy.
Created 08/21/20; re-posted 03/12/21; updated (post title changed, new articles added) 01/14/22.
