Velchev JD, Van Laer L, Luyckx I, Dietz H, Loeys B. Loeys-Dietz Syndrome. Adv Exp Med Biol. 2021;1348:251-264. Full-text for Emory users.
From: Table 11.1. Clinical features at initial diagnosis of LDS. (Velchev JD, et al., p. 253.)
- Vascular findings
- Arterial tortuosity 92%
- Most common in head and neck vessels
- Carotids (55%)
- Vertebral (56%)
- Intracranial (37%)
- Ascending aorta (5%), aortic arch (10%)
- Descending thoracic (4%) or abdominal
- (7%) Ao, also other vessels (e.g. iliacs)
- Most common in head and neck vessels
- Arterial tortuosity 92%
- Aneurysms
- Aorta
- Root 87%
- Ascending 27%
- Arch 10%
- Desc thoracic 15%
- Abdominal 12%
- Vessel beyond Ao 30%
- Aorta

(Velchev JD, et al., p. 256.)
Loeys BL, Dietz HC. Loeys-Dietz Syndrome. 2008 Feb 28 [Updated 2018 Mar 1]. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet].
“Individuals with LDS have a more aggressive vascular course (with routine involvement of vascular segments distant from the aortic root) than that observed in Marfan syndrome. Mean age at death is 26 years [Loeys et al 2006]. Attias et al [2009] reported that the proportion of individuals with aortic dilatation, the age at dissection, and the need for surgery were similar in those with a heterozygous TGFBR2 pathogenic variant and those with a heterozygous FBN1 pathogenic variant causative of Marfan syndrome; however, the rate of death was greater in families with a heterozygous TGFBR2 pathogenic variant. Similarly, a study of 228 families with a heterozygous pathogenic variant in either TGFBR1 or TGFBR2 demonstrated similar aortic risk (dissection or aortic surgery) in both groups [Jondeau et al 2016].” (Loeys, et al., p. 10-11.)
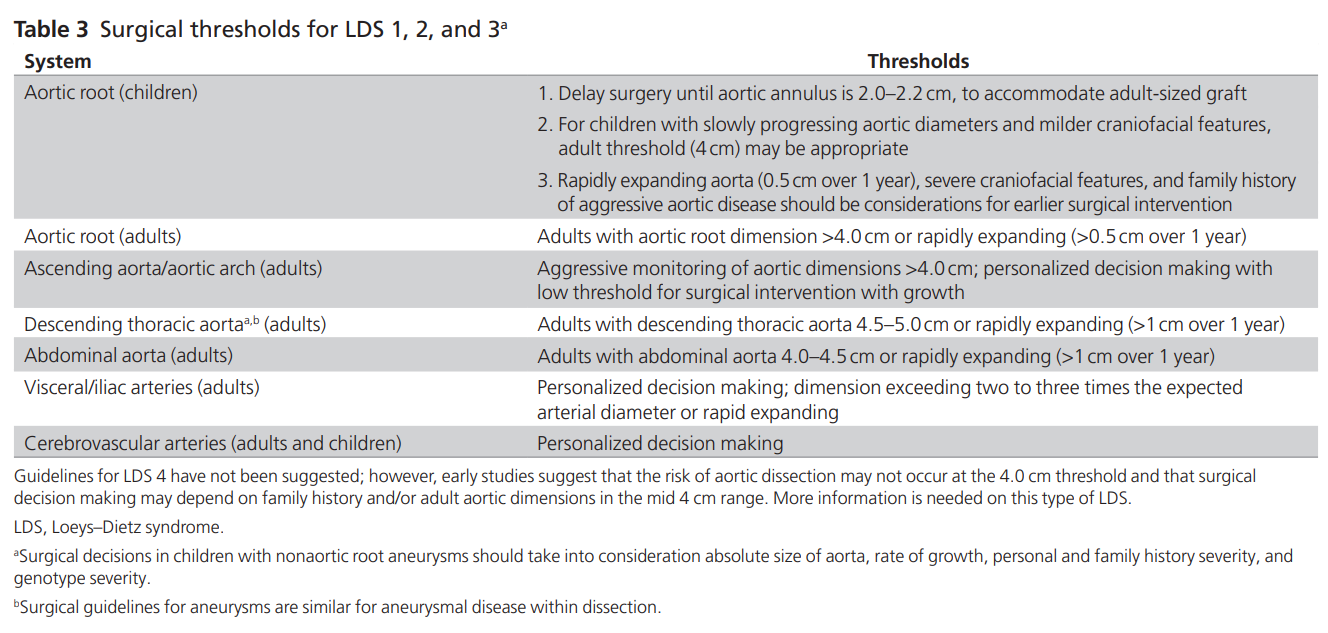
MacCarrick G, Black JH 3rd, Bowdin S, El-Hamamsy I, Frischmeyer-Guerrerio PA, Guerrerio AL, Sponseller PD, Loeys B, Dietz HC 3rd. Loeys-Dietz syndrome: a primer for diagnosis and management. Genet Med. 2014 Aug;16(8):576-87. doi: 10.1038/gim.2014.11. Free full-text.