
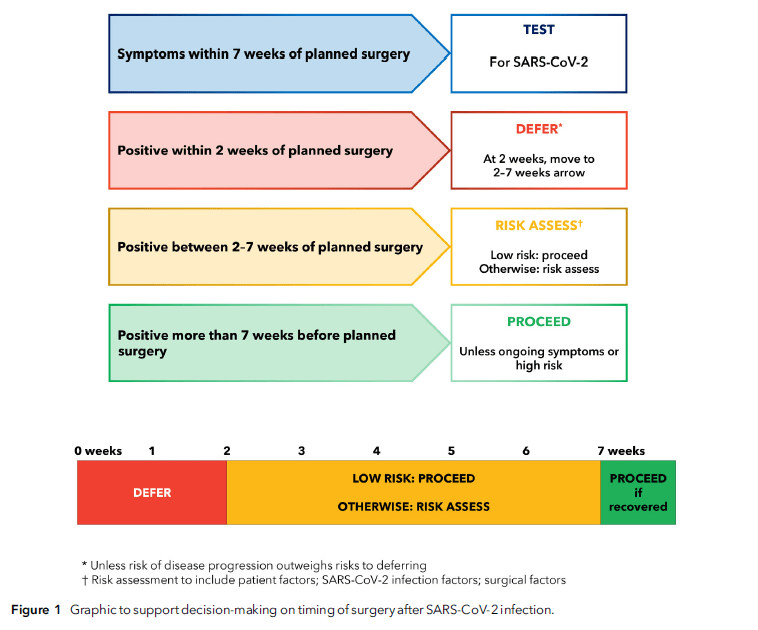
“Patients who develop symptoms of SARS-CoV-2 infection within 7 weeks of planned surgery, including on the day of surgery, should be screened for SARS-CoV-2. Elective surgery should not usually be undertaken within 2 weeks of diagnosis of SARS-CoV-2 infection. For patients who have recovered from SARS-CoV-2 infection and who are low risk or having low-risk surgery, most elective surgery can proceed 2 weeks following a SARS-CoV-2 positive test. For patients who are not low risk or having anything other than low-risk surgery between 2 and 7 weeks following infection, an individual risk assessment must be performed. This should consider: patient factors (age; comorbid and functional status); infection factors (severity; ongoing symptoms; vaccination); and surgical factors (clinical priority; risk of disease progression; grade of surgery).”
“This guidance document supports more general clinical guidance on risk assessment prior to surgery: decision-making should be shared, individualised and consider the balance of risk associated with proceeding with surgery as planned, against other options. As is the case with most other risk factors which could be reduced or optimized over time, the risks of proceeding without delay will depend on the patient’s other risk factors and magnitude and urgency of the surgery planned.”
El-Boghdadly, K et al. “Timing of elective surgery and risk assessment after SARS-CoV-2 infection: 2023 update: A multidisciplinary consensus statement on behalf of the Association of Anaesthetists, Federation of Surgical Specialty Associations, Royal College of Anaesthetists and Royal College of Surgeons of England.” Anaesthesia vol. 78,9 (2023): 1147-1152. Free Full Text.
