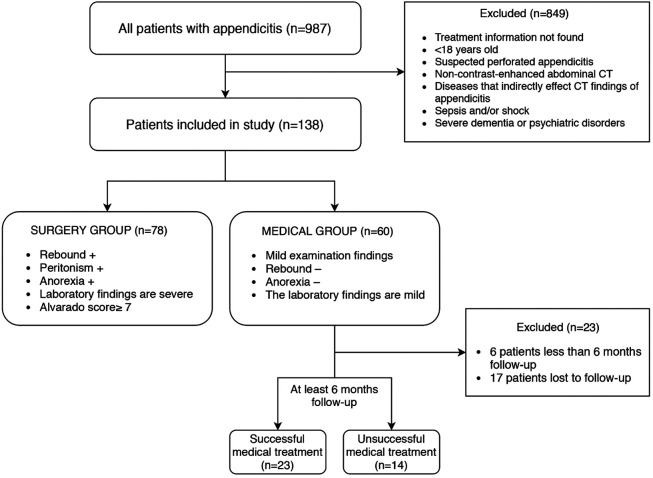
“Although medical treatment has proven to be a successful method of treatment of uncomplicated acute appendicitis, there is still controversy over which treatment to apply. It is intended that the computed tomography (CT) appendicitis score, which carries the information of all CT parameters, gives us an idea about the severity of acute appendicitis, such as the Alvarado score.”
“A retrospective analysis was conducted on 138 patients with acute appendicitis who underwent CT between 2015 and 2019. In this study, medical treatment group (n = 60) versus surgical treatment group (n = 78) and successful antibiotic treatment group (n = 23) versus unsuccessful antibiotic treatment group (n = 14) were compared.”
“Preoperative CT quite consistently has been shown to lower the negative appendectomy rate among women. Relatively few studies, however, have shown a lower negative appendectomy rate with preoperative CT for both sexes. Furthermore, any suggested utility of preoperative CT in men is contradicted by a number of studies that have shown that men derive no benefit from preoperative CT when there is clinical suspicion of acute appendicitis. Nevertheless, CT is used routinely among men with suspected appendicitis at our institution and has been assumed by both surgeons and radiologists to be a useful practice. Therefore, we performed this study to determine the negative appendectomy rates of patients who did and did not undergo preoperative CT and to determine, more specifically, whether men benefit from preoperative CT.”
Negative Appendectomy Rates for Patients Who Did and Did Not Undergo Preoperative ImagingContinue reading →
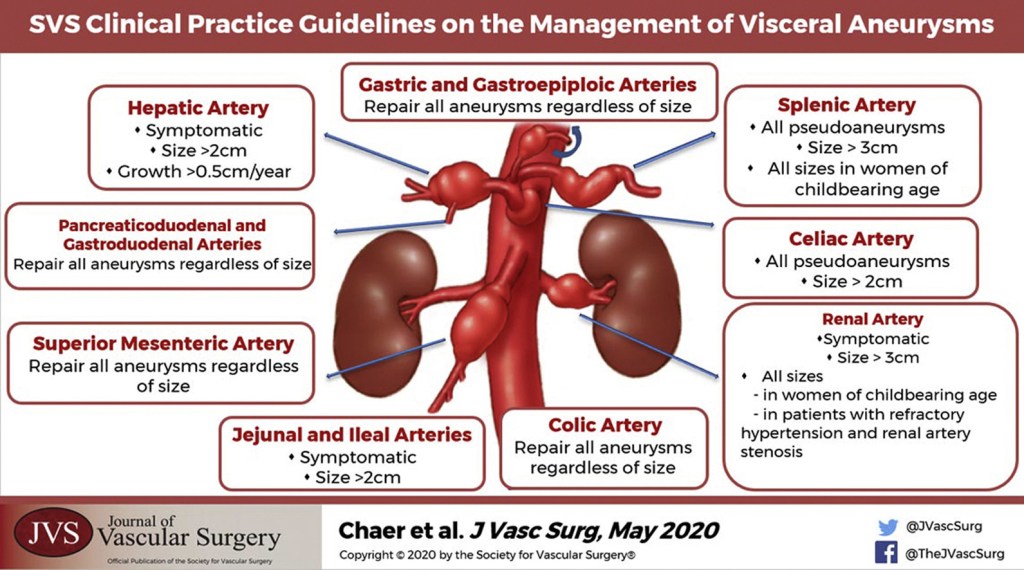
“Although not directed by randomized prospective trials, general principles of management of visceral artery aneurysms do exist. Because of their potential for rupture, most visceral artery pseudoaneurysms, mycotic aneurysms, and many larger true aneurysms warrant intervention. Treatment can generally be accomplished by either open surgical or endovascular approaches. The treatment goal is to prevent aneurysm expansion and potential rupture by exclusion from the arterial circulation while maintaining necessary distal or collateral bed perfusion. Depending on the location of the aneurysm, this can be accomplished in a variety of ways. In areas of the visceral circulation with an abundance of collateral flow, for example, in the splenic artery, proximal and distal ligation of the aneurysm segment is a viable surgical option. This can also be accomplished with endovascular isolation of the aneurysmal segment, either by placement of a stent graft or by coil embolization of the proximal and distal arterial segment. The preferred treatment of an individual patient and aneurysm must be carefully based on the particular anatomy and any associated clinical conditions as well as the underlying condition of the patient. The purpose of these guidelines is to inform the diagnosis, treatment options, screening, and follow-up of visceral aneurysms based on the available published literature and the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach”
“Recent reports by the Australian Safety and Efficacy Register for New interventions and Procedures (ASERNIP-S) and the Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) concluded that insufficient evidence is available to assess the safety of the open versus closed laparoscopy in regard to major vascular and visceral injuries.” (Larobina & Nottle)
Major Vascular Injuries in Closed vs. Open Laparoscopy (Larobina & Nottle)
“Our case series shows that open laparoscopy can vastly reduce the incidence of access-related morbidity and mortality. Only a single visceral injury occurred in 5900 cases, and no major vascular injuries were reported.These figures are consistent with those of other reported series of open laparoscopy, which also show a zero rate of vascular injury and low rates of visceral injury.The literature review showed a rate of 1 injury to major retroperitoneal vessels per 2272 cases of closed laparoscopy procedures. This compares with a major vascular injury rate of 0 for the open technique. This difference is both statistically significant ( P = 0.003) and highly clinically significant.” (Larobina & Nottle)
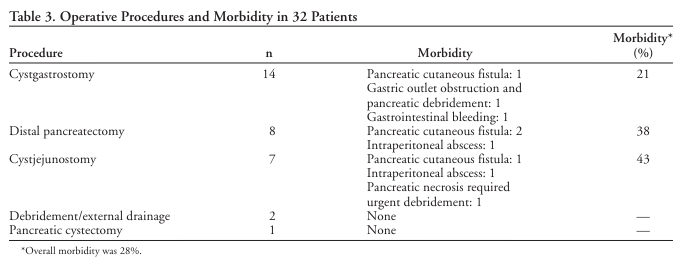
“Operative internal drainage has been standard treatment for chronic unresolved pancreatic pseudocysts (PPs). Recently, percutaneous external drainage (PED) has become the primary mode of treatment at many medical centers.”
“ Operative management for PPs appears to be superior to CT-guided PED. Although the later was often successful, it required major salvage procedures in one third of the patients. An expectant management protocol may be suitable for selected patients.”
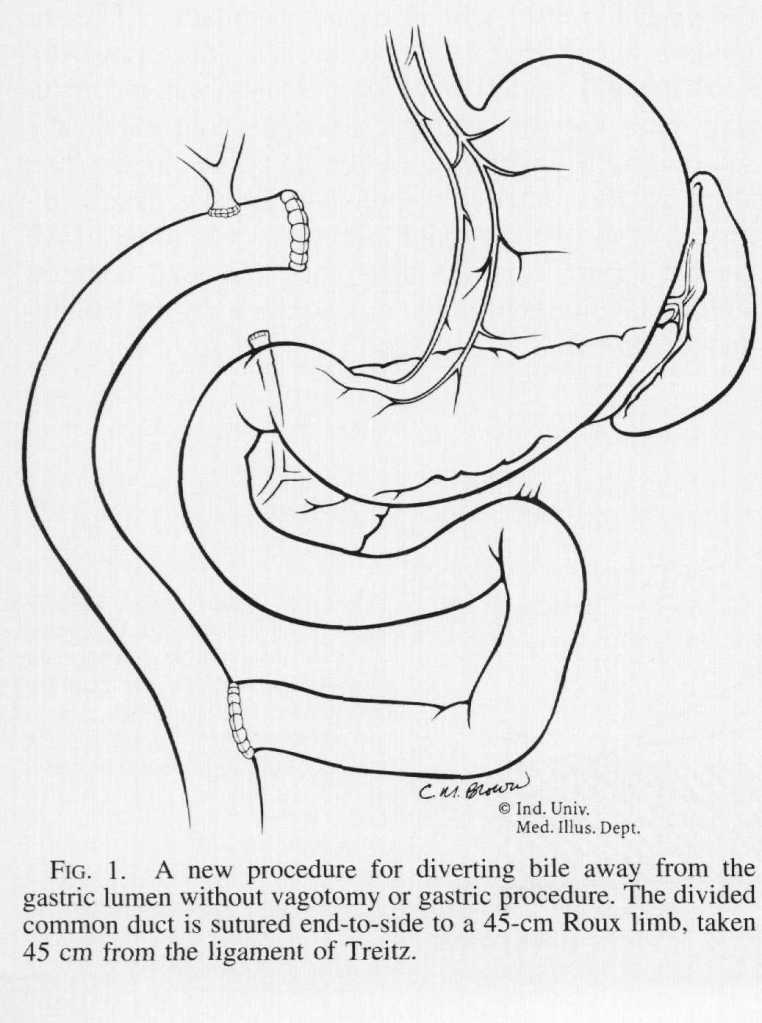
“Various treatments for [Primary Bile Reflux Gastritis] have been proposed since its recognition. Operations that have been utilized are the Roux-en-Y procedure, the Braun enteroenterostomy, the Henley jejunal interposition, and several modifications of each of these operations. These procedures produce relief from bile reflux, but all have particular side effects of their own. Before the utilization of vagotomy for ulcer disease, stomal ulceration at the gastrojejunal anastomosis was the most frequent postoperative problem. Currently, the most commonly applied operation is the Roux-en-Y gastrojejunostomy, which requires vagotomy and antrectomy and results in the equally disabling Roux stasis syndrome in about one-half of patients.”
“Because of these difficulties, a new procedure is proposed wherein only bile is diverted by means of a Roux-en-Y limb and no gastric procedure is done. This allows minimal disturbance of gastric motility and totally diverts bile away from the gastric lumen.”
“Popliteal artery aneurysms (PAAs) are the most common peripheral arterial aneurysms, defined as aneurysms outside the aortoiliac system or the brain, accounting for 70% of all peripheral arterial aneurysms. They are more common in men (95%) and tend to occur in the sixth and seventh decades of life. Few modern studies have been performed on the natural history of PAAs, and many of these were retrospective reviews of surgical patients. As such, the timing and details of PAA management remain nuanced.”
“These guidelines focus on PAA screening, indications for intervention, choice of repair strategy, management of asymptomatic and symptomatic PAAs (including those presenting with acute limb ischemia), and follow-up of both untreated and treated PAAs. They offer long-awaited evidence-based recommendations for physicians taking care of these patients.”