
Hassold N, et al. Effectiveness and outcome of endovascular therapy for late-onset postpancreatectomy hemorrhage using covered stents and embolization. J Vasc Surg. 2016 Nov;64(5):1373-1383.
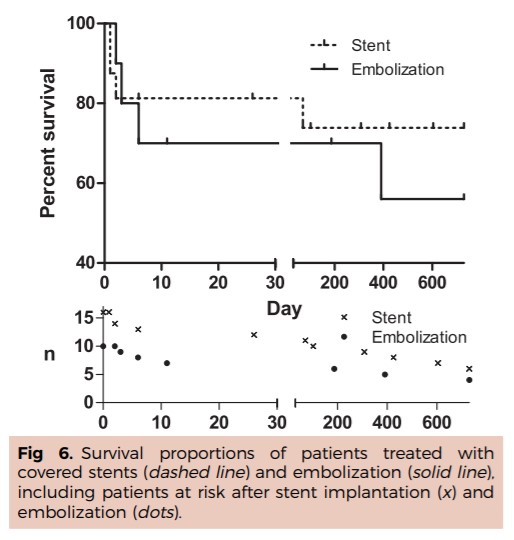
RESULTS: Covered stent placement was successful in 14 of 16 patients (88%); embolization was successful in 10 of 11 (91%) patients. For the embolization group, the overall 30-day and 1-year survival rate was 70%, and the 1- and 2-year survival rate was 56%; for the covered stent group, these rates were 81% and 74%, respectively. The 30-day patency of the covered stent was 84%, and 1-year patency was 42%; clinically relevant ischemia was observed in two patients. Infarction distal to the embolized vessel occurred in 6 of 11 patients (55%).
CONCLUSIONS: Endovascular treatment using either covered stents or embolization techniques is an effective and safe emergency therapy for life-threatening postpancreatectomy hemorrhage with good clinical success rates and long-term results. Covered stent placement preserving vessel patency in the early postoperative phase should be preferred to embolization if it is technically feasible.
Ching KC, et al. Covered Stents and Coil Embolization for Treatment of Postpancreatectomy Arterial Hemorrhage. J Vasc Interv Radiol. 2016 Jan;27(1):73-9.
Full-text for Emory users.
RESULTS: Median onset of hemorrhage was at 39 days (mean, 27.9 d; range, 5-182 d). Covered stents were used in 65.7% of interventions, coil embolization in 23.6%, stent-assisted embolization in 5.2%, and stent-graft angioplasty in 2.6%. A total of 28 stent-grafts were placed, of which 19 were self-expandable and nine were balloon-mounted. Mean stent-graft diameter was 6.6 mm (range, 5-10 mm). Recurrent bleeding occurred following 26.3% of interventions in seven patients at a mean interval of 22 days. The site of recurrent bleeding was new in 80% of cases. There was no significant difference in recurrent bleeding rate in early-onset (< 30 d; n = 22) versus late-onset PPAH (> 30 d; n = 6; P > .05). No ischemic hepatic or bowel complications were identified. The 30-day mortality rate was 7.1% (n = 2) and was significantly higher in patients with initial PPAH at ≥ 39 days (n = 5; P = .007).
CONCLUSIONS: Covered stents and coil embolization are effective for managing PPAH and maintaining distal organ perfusion to minimize morbidity and mortality. Recurrent bleeding is common and most often occurs from new sites of vascular injury rather than previously treated ones.
Khalsa BS, et al. Evolution in the Treatment of Delayed Postpancreatectomy Hemorrhage: Surgery to Interventional Radiology. Pancreas. 2015 Aug;44(6):953-8.
Full-text for Emory users.
 TABLE 1. Summary of Results of Patients With Postpancreatectomy Hemorrhage After Pancreaticoduodenectomy
TABLE 1. Summary of Results of Patients With Postpancreatectomy Hemorrhage After Pancreaticoduodenectomy
RESULTS: Management evolved from operative intervention alone, to combined operative and on-table angiographic intervention, to endovascular intervention alone. The prevalence of PPH was 3.0%. Delayed PPH occurred with a mean of 13.8 days. On angiography, visceral arteries affected were the gastroduodenal artery, hepatic artery, jejunal branches of the superior mesenteric artery, pancreaticoduodenal artery, and inferior phrenic artery. Ninety-day mortality for PPH was 20%. From early to recent experience, the mortality rate was 100% for operative intervention alone, 25% for combined operative and on-table angiographic intervention, and 0% for endovascular intervention alone.
CONCLUSIONS: Our 10-year experience supports current algorithms in the management of PPH. Key considerations include the recognition of the sentinel bleed, the presence of a pancreatic fistula, and the initial operative role of a long gastroduodenal artery stump with radiopaque marker for safe and effective embolization should PPH occur.
More PubMed results for stents and coils for PPH.
