
Gandhi D, et al. Solid pseudopapillary Tumor of the Pancreas: Radiological and surgical review. Clin Imaging. 2020 Nov;67:101-107.
Full-text for Emory users.
Highlights:
- Solid Pseudopapillary Neoplasms of the pancreas are rare pancreatic tumors with low grade malignant potential, typically affecting young females.
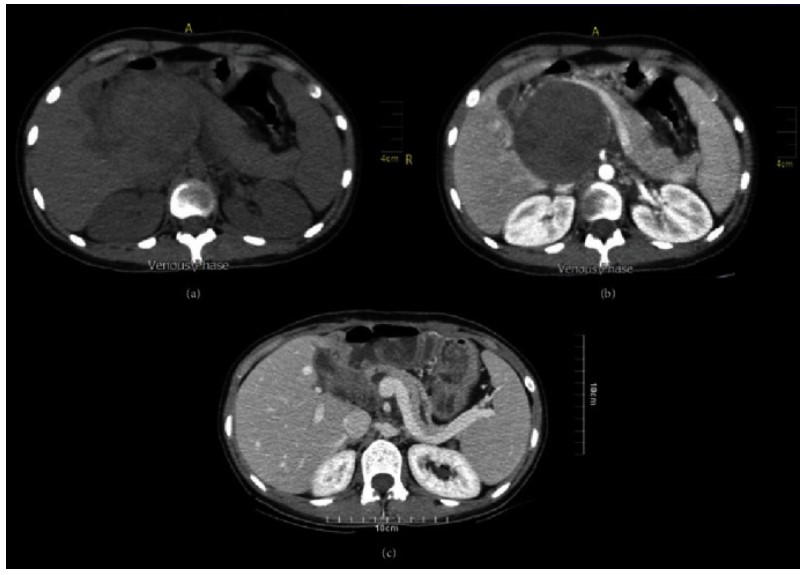
- Small SPNs (< 3cm in diameter) usually appear as completely solid tumors with sharp margins and gradually enhancing, well encapsulated masses in the pancreas and may demonstrate varying amounts of hemorrhage.
- Large lesions have mixed solid – cystic components showing early weak enhancement with gradual increase in enhancement in the hepatic venous phase.
- Atypical features including extracapsular, as well as parenchymal invasion, simulation of islet cell tumors, calcifications, ductal obstruction, and metastasis are suspicious for malignant degradation.
- The tumor is considered unresectable in the event that it invades or encases the aorta, encases >180 degree of the SMA regardless of tumor location in the pancreas, abuts the celiac artery (when the tumor is located in the pancreatic head) or encases >180 degree of the celiac artery (when the tumor is located in the body/tail of the pancreas).

Tjaden C, et al. Outcome and prognosis after pancreatectomy in patients with solid pseudopapillary neoplasms. Pancreatology. 2019 Jul;19(5):699-709.
Full-text for Emory users.
Results: Fifty-two patients were identified, 44 (85%) of them were female and the median age was 29 years (IQR 9-71). Seven (13%) patients showed a malignant behaviour of SPN with N1 (n = 2) or M1 (n = 1) disease at resection; 5 patients developed tumor recurrence, after a median of 21 months. During follow-up time (median 54 months) all patients were alive, the 5- and 10-year rates for disease-free survival were 89.0% and 81.6%, respectively. Significant risk factors for recurrence were age <18 years (p = 0.0087) and parenchyma-preserving surgical approaches (p = 0.0006). The postoperative long-term outcome showed ECOG = 0-1 in all patients, with resection related exocrine insufficiency in 20 (41%) and diabetes mellitus in 2 (4%) patients.
Conclusions: Age < 18 years is a significant risk factor for malignancy in SPN, and parenchyma preserving resections harbor a significant risk for tumor recurrence. As recurrence may occur late, a systematic life-long follow-up should be performed.
Dalili A, et al. Solid Pseudopapillary Neoplasms Are Rare, Indolent Pancreatic Tumors in Young Women. Case Rep Surg. 2020 Nov 23;2020:6694904.
“Surgical resection has continuously been the treatment of choice for SPN patients; however, the location, size, and the local invasion of the tumor determine the surgical technique [1]. Depending on the tumor’s location, pancreaticoduodenectomy is indicated for a tumor in the head of the pancreas, distal pancreatectomy for tail lesions, and the tumors in the neck and body can be treated by central pancreatectomy [12]. Recently, laparoscopic procedures and the parenchyma-preserving surgical approach are discussed in many pieces of literature [12, 13, 17–19]. Hao et al. recommended minimally invasive surgery for SPN of the proximal pancreas due to some convinced aspects like shorter hospitalization, decreased blood loss, and less transfusion requirement than open surgery [10, 17].” (Dalili, 2020, p. 3)
Marchegiani G, et al. Solid pseudopapillary tumors of the pancreas: Specific pathological features predict the likelihood of postoperative recurrence. J Surg Oncol. 2016 Oct;114(5):597-601.

Results: The majority of patients were female (86.3%) with a median age of 33 (7-68) years. The prevalent location was the pancreatic tail (33.5%). Applying the WHO criteria, 16 (12.2%) SPTs were considered malignant due to the presence of at least pancreatic parenchyma (9.9%), perineural (4.6%), and/or angiovascular invasion (2.3%). After a median of 62 months after surgery, only two patients had a recurrence (1.5%). Both of them fulfilled the WHO criteria for malignant SPT (vs. 10.7% of those who did not recur, P = 0.01), had an infiltrative growth pattern (vs. 10.8%, P = 0.01), pancreatic parenchyma invasion (vs. 9.7%, P = 0.01) and capsular invasion (vs. 4.9%, P = 0.004).
Conclusion: Overall, SPTs are associated with excellent survival results after surgical resection. Disease recurrence is extremely rare, and might occur if the primary tumor presents with either pancreatic parenchyma or capsule invasion.
More PubMed results on surgical management of SPNs.
