
Oberkofler CE, et al. A multicenter randomized clinical trial of primary anastomosis or Hartmann’s procedure for perforated left colonic diverticulitis with purulent or fecal peritonitis. Ann Surg. 2012 Nov; 256(5):819-26; discussion 826-7.
Full-text for Emory users.
Results: Patient demographics were equally distributed in both groups (Hinchey III: 76% vs 75% and Hinchey IV: 24% vs 25%, for HP vs PA, respectively). The overall complication rate for both resection and stoma reversal operations was comparable (80% vs 84%, P = 0.813). Although the outcome after the initial colon resection did not show any significant differences (mortality 13% vs 9% and morbidity 67% vs 75% in HP vs PA), the stoma reversal rate after PA with diverting ileostomy was higher (90% vs 57%, P = 0.005) and serious complications (Grades IIIb-IV: 0% vs 20%, P = 0.046), operating time (73 minutes vs 183 minutes, P < 0.001), hospital stay (6 days vs 9 days, P = 0.016), and lower in-hospital costs (US $16,717 vs US $24,014) were significantly reduced in the PA group.
Conclusions: This is the first randomized clinical trial favoring PA with diverting ileostomy over HP in patients with perforated diverticulitis.
Thornell A, et al. Laparoscopic Lavage for Perforated Diverticulitis With Purulent Peritonitis: A Randomized Trial. Ann Intern Med. 2016 Feb 2;164(3):137-45.
Full-text for Emory users.
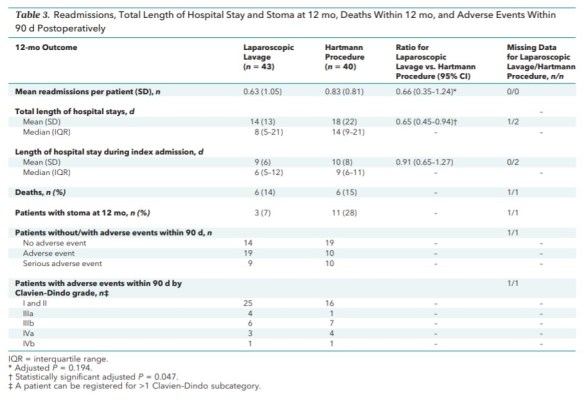
A total of 43 and 40 patients were randomly assigned to laparoscopic lavage and the Hartmann procedure with a median (first, third quartiles) follow-up of 372 days (336, 394) and 378 days (226, 396), respectively. Fewer patients in the laparoscopic group (12 of 43; 27.9%) than in the Hartmann group (25 of 40; 62.5%) had at least 1 reoperation within 12 months (relative risk reduction, 59%; relative risk, 0.41 [95% CI, 0.23 to 0.72]; P = 0.004). Mortality and severe adverse events did not differ between groups. Total length of hospital stay (days) within 12 months was shorter for the laparoscopic group than the Hartmann group, with a reduction of 35% (relative risk, 0.65 [CI, 0.45 to 0.94]; P = 0.047). After 12 months, 3 patients in the laparoscopic group and 11 in the Hartmann group had a stoma.
Lambrichts DPV, et al. Hartmann’s procedure versus sigmoidectomy with primary anastomosis for perforated diverticulitis with purulent or faecal peritonitis (LADIES): a multicentre, parallel-group, randomised, open-label, superiority trial. Lancet Gastroenterol Hepatol. 2019 Aug;4(8):599-610.
Full-text for Emory user.
Findings: Between July 1, 2010, and Feb 22, 2013, and June 9, 2013, and trial termination on June 3, 2016, 133 patients (93 with Hinchey III disease and 40 with Hinchey IV disease) were randomly assigned to Hartmann’s procedure (68 patients) or primary anastomosis (65 patients). Two patients in the Hartmann’s group were excluded, as was one in the primary anastomosis group; the modified intention-to-treat population therefore consisted of 66 patients in the Hartmann’s procedure group (46 with Hinchey III disease, 20 with Hinchey IV disease) and 64 in the primary anastomosis group (46 with Hinchey III disease, 18 with Hinchey IV disease). In 17 (27%) of 64 patients assigned to primary anastomosis, no stoma was constructed. 12-month stoma-free survival was significantly better for patients undergoing primary anastomosis compared with Hartmann’s procedure (94·6% [95% CI 88·7-100] vs 71·7% [95% CI 60·1-83·3], hazard ratio 2·79 [95% CI 1·86-4·18]; log-rank p<0·0001). There were no significant differences in short-term morbidity and mortality after the index procedure for Hartmann’s procedure compared with primary anastomosis (morbidity: 29 [44%] of 66 patients vs 25 [39%] of 64, p=0·60; mortality: two [3%] vs four [6%], p=0·44).
Interpretation: In haemodynamically stable, immunocompetent patients younger than 85 years, primary anastomosis is preferable to Hartmann’s procedure as a treatment for perforated diverticulitis (Hinchey III or Hinchey IV disease).
More PubMed results on management of perforated diverticulitis.
