“Acute perforated diverticulitis with peritonitis is a feared complication of diverticular disease. The incidence in Western countries is estimated to be 1.85 per 100 000 population per year for purulent peritonitis. Even with optimal treatment, perforated diverticulitis has a high morbidity and mortality. Traditionally, the standard treatment has been emergency surgery with resection of the diseased bowel, often with colostomy creation. Studies have indicated that laparoscopic lavage with drainage and antibiotics might be a treatment option in perforated diverticulitis. So far, 3 European randomized clinical trials have shown somewhat different results, and no clear advantages have been demonstrated with laparoscopic lavage, except a lower stoma rate at 1-year follow-up. Nine meta-analyses and systematic reviews of the short-term and 1-year results of these trials have been published in the last 4 years, with divergent conclusions. No long-term results on laparoscopic lavage have yet been published.”
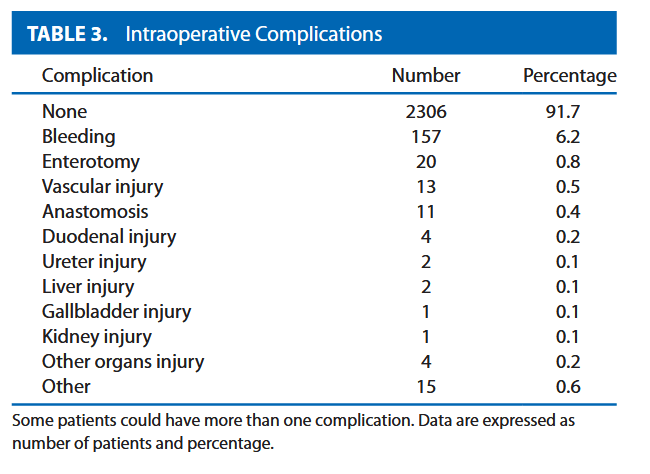
“Right hemicolectomy is considered one of the simplest colorectal major procedures and is often considered an appropriate first step for residents and young fellows. Despite this, complications after right hemicolectomy for cancer are common, at ≈30%, and postoperative mortality is reported to be ≈3%. Anastomotic leak (AL) after right hemicolectomy for cancer is a major contributor to this short-term morbidity and mortality. The document AL rate after right hemicolectomy ranges widely, from 1.3% to 8.4%. This also has a significant impact on healthcare costs and major oncologic consequences, as demonstrated by the higher cancer recurrence rate after AL.”
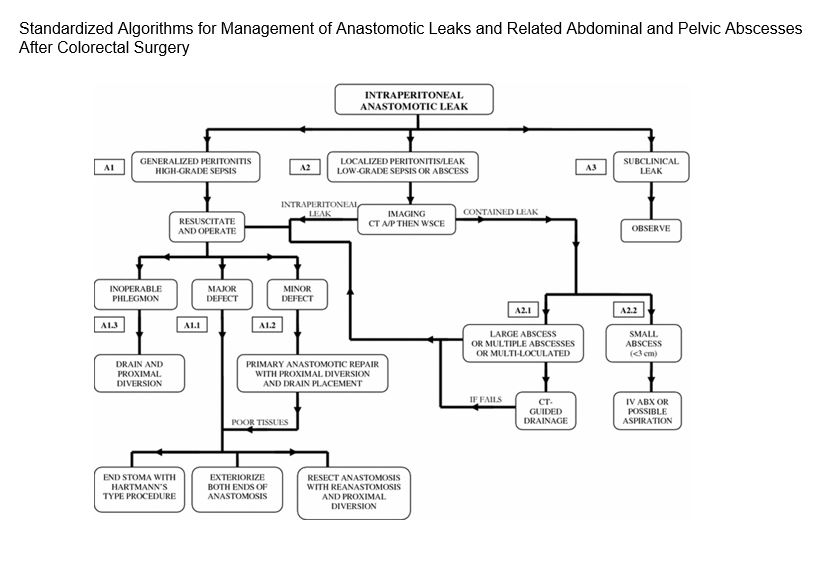
“The risk factors and incidence of anastomotic leak following colorectal surgery are well reported in the literature. However, the management of the multiple clinical scenarios that may be encountered has not been standardized.” In this study, “management scenarios were divided into those for intraperitoneal anastomoses, extraperitoneal (low pelvic) anastomoses, and anastomoses with proximal diverting stomas. Management options were then based on the clinical presentation and radiographic findings and organized into three interconnected algorithms.”
Recommendations for the management of intraperitoneal anastomotic leak with references to the pertinent sections of this article for more information. KEY: IV ABX=intravenous antibiotics; CT=computed tomographic; WSCE=water soluble contrast enema; CT A/P=computed tomographic scan of the abdomen and pelvisContinue reading →
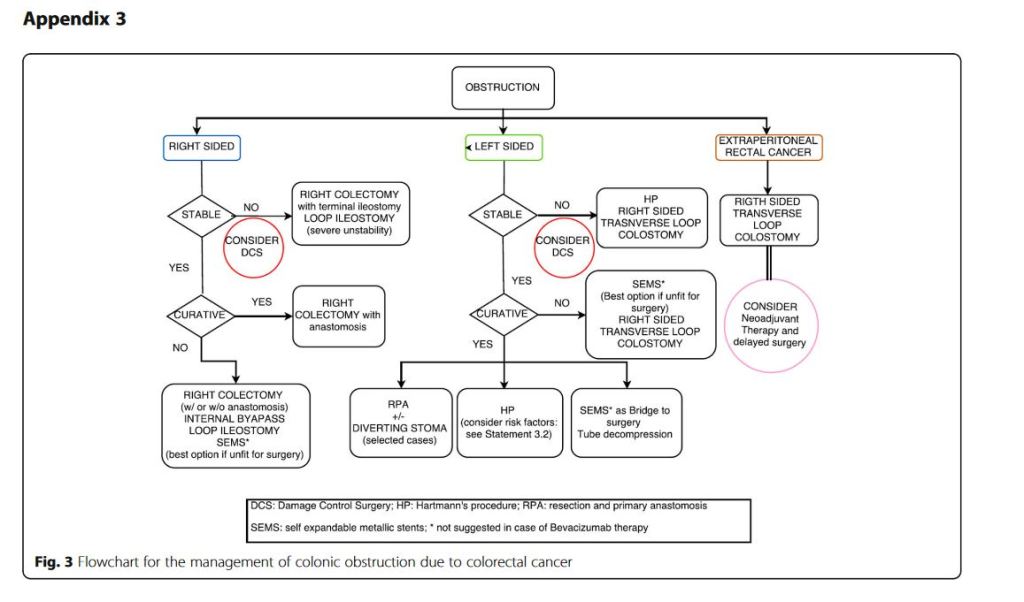
“Obstruction and perforation due to colorectal cancer represent challenging matters in terms of diagnosis, life-saving strategies, obstruction resolution and oncologic challenge. The aims of the current paper are to update the previous WSES guidelines for the management of large bowel perforation and obstructive left colon carcinoma (OLCC) and to develop new guidelines on obstructive right colon carcinoma (ORCC).” “CT scan is the best imaging technique to evaluate large bowel obstruction and perforation. For OLCC, self-expandable metallic stent (SEMS), when available, offers interesting advantages as compared to emergency surgery; however, the positioning of SEMS for surgically treatable causes carries some long-term oncologic disadvantages, which are still under analysis. In the context of emergency surgery, resection and primary anastomosis (RPA) is preferable to Hartmann’s procedure, whenever the characteristics of the patient and the surgeon are permissive. Right-sided loop colostomy is preferable in rectal cancer, when preoperative therapies are predicted. With regards to the treatment of ORCC, right colectomy represents the procedure of choice; alternatives, such as internal bypass and loop ileostomy, are of limited value.”
“Conclusions: grey areas and opportunities for improvements
We found some limitations within the present guidelines:
– They fail to cover all the possible abdominal scenarios when colon cancer occurs as an emergency: for example, associated resections were not taken into considerations, neither we discussed about therapeutic strategies in case of evidence of peritoneal carcinomatosis. – Despite our attempts to underline suggestions in case of low technical resources, the present guidelines are generally oriented toward hospitals with high level of resources.
On the other side, in our opinion, the current guidelines suggest some stimuli for doctors involved in this field:
– To review the approach to patient suffering from abdominal pain by introducing and promoting the use of bedside abdominal US. – To bear in mind that the emergency surgeon should have a strong oncologic background or that the specialised colorectal surgeon should have a strong background of surgical pathophysiology, emergency surgery and damage control philosophy. – To promote the use of clinical pathways within singular Hospitals”
Results: After randomization, 12 patients were excluded. Accordingly, 240 patients were included in the analysis; 118 were in the study group, and 122 in the control group. ICG angiography showed insufficient perfusion of the colic stump, which led to extended bowel resection in 13 cases (11%). An anastomotic leak developed in 11 patients (9%) in the control group and in 6 patients (5%) in the study group (p = n.s.).
Conclusions: Intraoperative ICG fluorescent angiography can effectively assess vascularization of the colic stump and anastomosis in patients undergoing colorectal resection. This method led to further proximal bowel resection in 13 cases, however, there was no statistically significant reduction of anastomotic leak rate in the ICG arm.
“This publication summarizes the changing treatment paradigm for patients with left-sided diverticulitis. Although diverticular disease can affect any segment of the large intestine, we will focus on left-sided disease. Bowel preparation, enhanced recovery pathways, and prevention of thromboembolic disease, while relevant to the management of patients with diverticulitis, are beyond the scope of these guidelines and are addressed in other ASCRS clinical practice guidelines.”
Results: Patient demographics were equally distributed in both groups (Hinchey III: 76% vs 75% and Hinchey IV: 24% vs 25%, for HP vs PA, respectively). The overall complication rate for both resection and stoma reversal operations was comparable (80% vs 84%, P = 0.813). Although the outcome after the initial colon resection did not show any significant differences (mortality 13% vs 9% and morbidity 67% vs 75% in HP vs PA), the stoma reversal rate after PA with diverting ileostomy was higher (90% vs 57%, P = 0.005) and serious complications (Grades IIIb-IV: 0% vs 20%, P = 0.046), operating time (73 minutes vs 183 minutes, P < 0.001), hospital stay (6 days vs 9 days, P = 0.016), and lower in-hospital costs (US $16,717 vs US $24,014) were significantly reduced in the PA group.
Conclusions: This is the first randomized clinical trial favoring PA with diverting ileostomy over HP in patients with perforated diverticulitis.