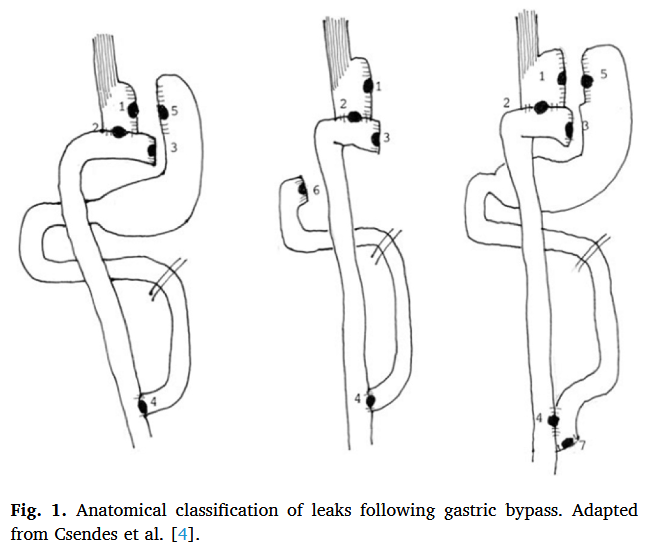
“Leaks and fistulas are among the most feared complications of bariatric surgery. Variable in presentation, acuity, and severity, these often require multimodal and multispecialty management strategies for optimal outcomes. Recent advancements in the realm of endoscopic therapies have made these integral to the treatment algorithm of post-operative leaks and fistulas. In this review, we will discuss the epidemiology, pathophysiology and classification of post-bariatric surgery defects and provide an in-depth assessment of current management strategies, with a focus on endoscopic therapies.”
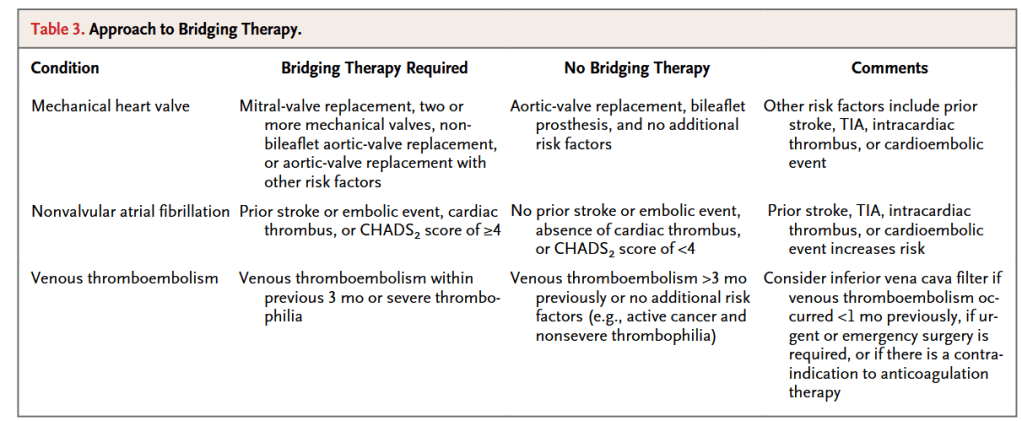
“The question of whether antithrombotic therapy should be suspended in a patient who will be undergoing an invasive procedure involves balancing the risk of postproce- dural bleeding with continued treatment against the thrombotic risk with suspension of treatment and use of bridging anticoagulation therapy. In general, a patient under- going a procedure that is associated with a low risk of bleeding (low-risk procedure) can safely continue antithrombotic therapy and should do so, particularly if the pa- tient is at high risk for a thromboembolic event (high-risk patient). Conversely, a pa- tient undergoing a high-risk procedure can temporarily discontinue antithrombotic agents safely if the patient is at low risk for a thromboembolic event (low-risk patient).”
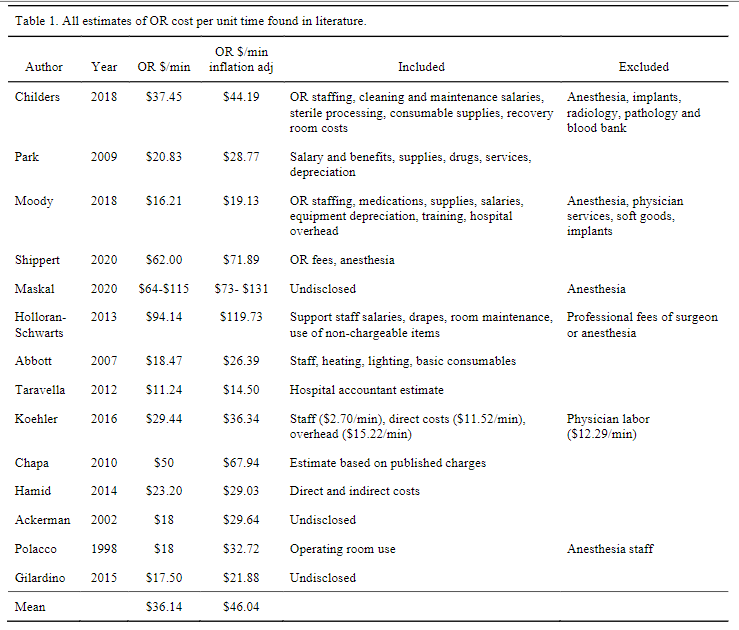
“The cost to run an operating room can be divided into direct costs such as staff wages and consumable items, indirect costs such as building maintenance, leasing/mortgage payments and laundry services, professional fees such as anesthesia and surgeon fees, and specialty service fees such as intraoperative fluoroscopy, blood bank, lab, and orthopaedic implants. Most of these figures can be estimated from purchase orders and salaries payable by hospital accounting systems. More recently, time driven activity-based costing (TDABC) has allowed a more accurate way to assign cost in a complex environment where staff are often multi-tasking and thousands of consumables are utilized. TDABC divides complex care into discrete cycles allowing micro-costing assessment and assignment of cost based ontime. In either of these methods, decisions must be made when attempting to measure and/or conceptualize the actual cost of a surgery. It should be noted that data in the current literature pertaining to the cost of the operating room often, but not always, excludes the costs associated with anesthesia services, perioperative services, surgeon fees, blood bank expenses, radiology services, and implants. Consistent data on operating room costs is needed for effective healthcare resource allocation.”
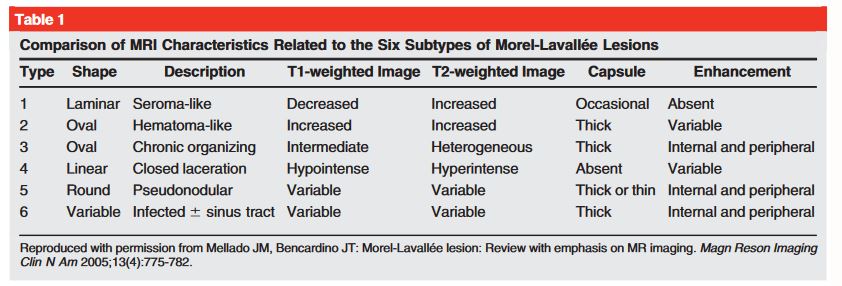
“The diagnosis of an MLL ideally is made by physical examination of the patient, but advanced imaging modalities can be used to provide additional information. Typically, CT of the area of interest is obtained, especially when a pelvic or acetabular injury is present. Small and large lesions often can be identified in this manner.”
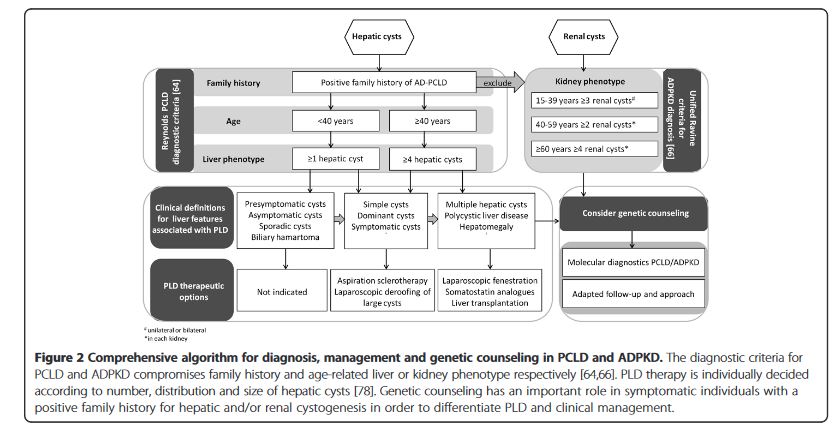
“Polycystic liver disease (PLD) is the result of embryonic ductal plate malformation of the intrahepatic biliary tree.The phenotype consists of numerous cysts spread throughout the liver parenchyma. Cystic bile duct malformations originating from the peripheral biliary tree are called Von Meyenburg complexes (VMC). In these patients embryonic remnants develop into small hepatic cysts and usually remain silent during life. Symptomatic PLD occurs mainly in the context of isolated polycystic liver disease (PCLD) and autosomal dominant polycystic kidney disease (ADPKD).” “Management of adult PLD is based on liver phenotype, severity of clinical features and quality of life. Conservative treatment is recommended for the majority of PLD patients. The primary aim is to halt cyst growth to allow abdominal decompression and ameliorate symptoms. Invasive procedures are required in a selective patient group with advanced PCLD, ADPKD or liver failure. Pharmacological therapy by somatostatin analogues lead to beneficial outcome of PLD in terms of symptom relief and liver volume reduction.”