
Selby R. “TEG talk”: expanding clinical roles for thromboelastography and rotational thromboelastometry. Hematology Am Soc Hematol Educ Program. 2020 Dec 4;2020(1): 67-75.
 Click to enlarge.
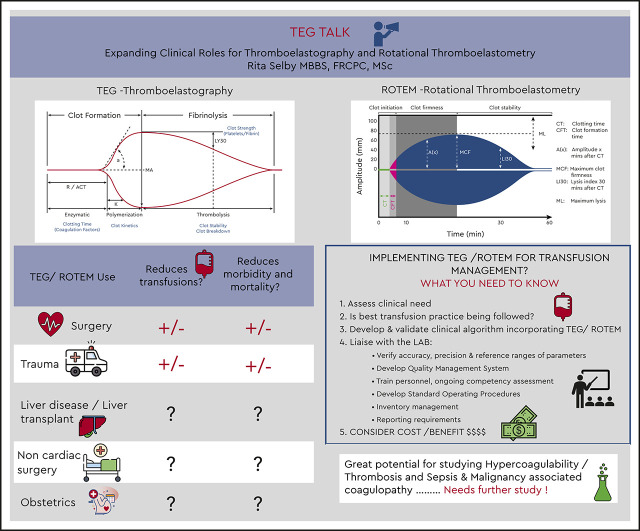
Click to enlarge. “Viscoelastic assays (VEAs) that include thromboelastography and rotational thromboelastometry add value to the investigation of coagulopathies and goal-directed management of bleeding by providing a complete picture of clot formation, strength, and lysis in whole blood that includes the contribution of platelets, fibrinogen, and coagulation factors. Conventional coagulation assays have several limitations, such as their lack of correlation with bleeding and hypercoagulability; their inability to reflect the contribution of platelets, factor XIII, and plasmin during clot formation and lysis; and their slow turnaround times. VEA-guided transfusion algorithms may reduce allogeneic blood exposure during and after cardiac surgery and in the emergency management of trauma-induced coagulopathy and hemorrhage. However, the popularity of VEAs for other indications is driven largely by extrapolation of evidence from cardiac surgery, by the drawbacks of conventional coagulation assays, and by institution-specific preferences. Robust diagnostic studies validating and standardizing diagnostic cutoffs for VEA parameters and randomized trials comparing VEA-guided algorithms with standard care on clinical outcomes are urgently needed. Lack of such studies represents the biggest barrier to defining the role and impact of VEA in clinical care.”
