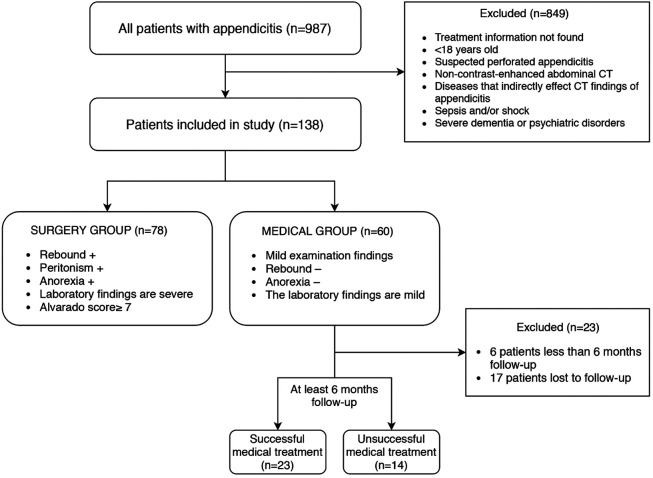
“Although medical treatment has proven to be a successful method of treatment of uncomplicated acute appendicitis, there is still controversy over which treatment to apply. It is intended that the computed tomography (CT) appendicitis score, which carries the information of all CT parameters, gives us an idea about the severity of acute appendicitis, such as the Alvarado score.”
“A retrospective analysis was conducted on 138 patients with acute appendicitis who underwent CT between 2015 and 2019. In this study, medical treatment group (n = 60) versus surgical treatment group (n = 78) and successful antibiotic treatment group (n = 23) versus unsuccessful antibiotic treatment group (n = 14) were compared.”
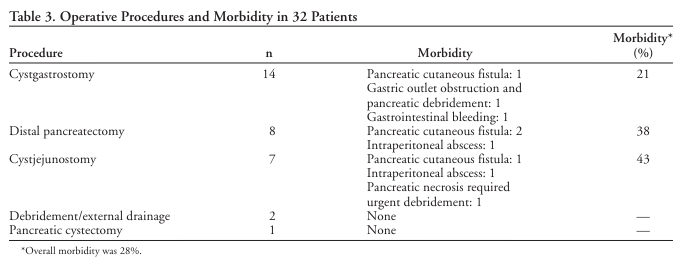
“Operative internal drainage has been standard treatment for chronic unresolved pancreatic pseudocysts (PPs). Recently, percutaneous external drainage (PED) has become the primary mode of treatment at many medical centers.”
“ Operative management for PPs appears to be superior to CT-guided PED. Although the later was often successful, it required major salvage procedures in one third of the patients. An expectant management protocol may be suitable for selected patients.”
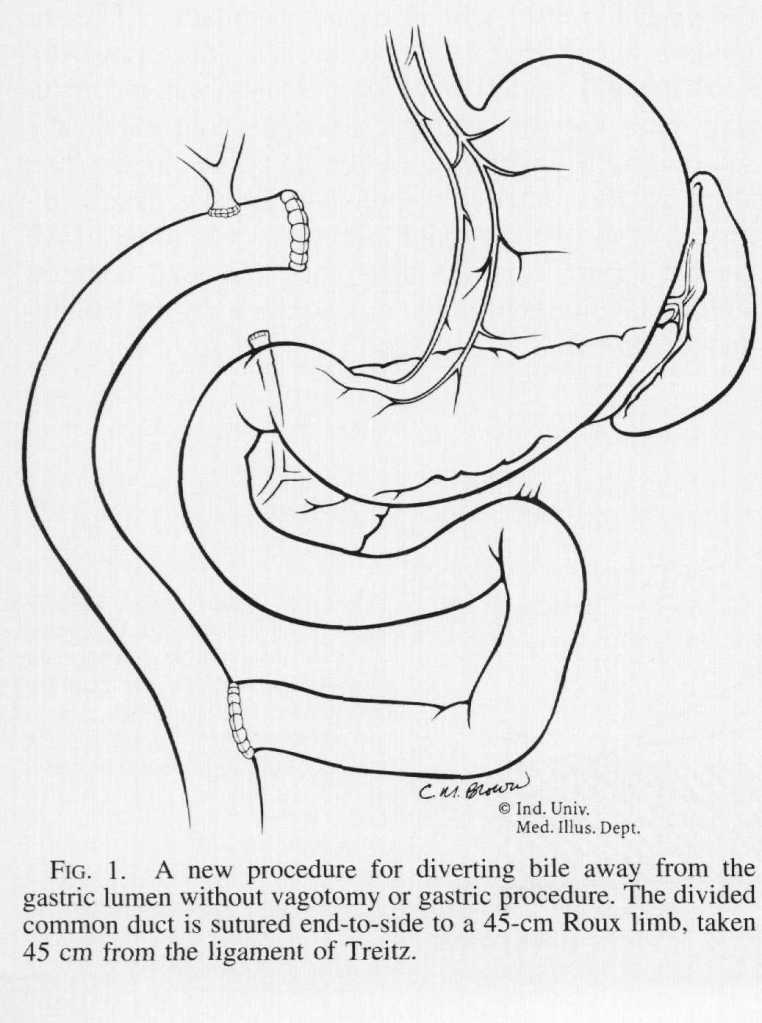
“Various treatments for [Primary Bile Reflux Gastritis] have been proposed since its recognition. Operations that have been utilized are the Roux-en-Y procedure, the Braun enteroenterostomy, the Henley jejunal interposition, and several modifications of each of these operations. These procedures produce relief from bile reflux, but all have particular side effects of their own. Before the utilization of vagotomy for ulcer disease, stomal ulceration at the gastrojejunal anastomosis was the most frequent postoperative problem. Currently, the most commonly applied operation is the Roux-en-Y gastrojejunostomy, which requires vagotomy and antrectomy and results in the equally disabling Roux stasis syndrome in about one-half of patients.”
“Because of these difficulties, a new procedure is proposed wherein only bile is diverted by means of a Roux-en-Y limb and no gastric procedure is done. This allows minimal disturbance of gastric motility and totally diverts bile away from the gastric lumen.”
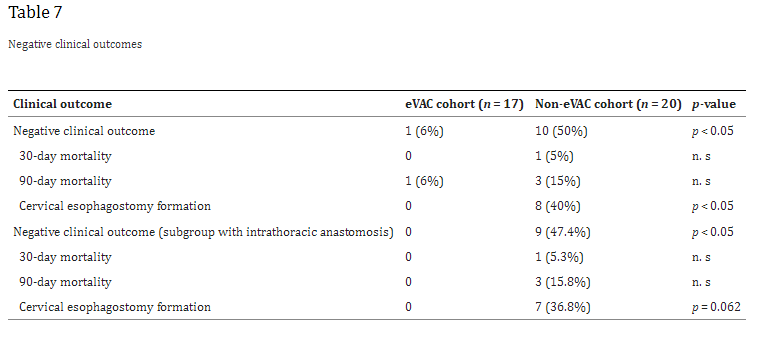
“Anastomotic leakages continue to be a highly challenging complication in esophageal surgery. According to the literature, the risk of anastomotic leakage after esophagectomy ranges between 4 and 35%. The location of the anastomotic leakage is a significant factor in determining patient outcomes. Notwithstanding, cervical anastomoses bear a higher risk for leakage; the consequences of an intrathoracic (mediastinal) leakage are usually more devastating. A leakage into the thoracic cavity typically leads to mediastinitis and severe pneumonia and contributes to the significant mortality rates in esophageal surgery. In contrast, cervical anastomotic leakages tend to frequently present as wound infections often only requiring external drainage”
“The clinical outcomes strongly depend on an early diagnosis and appropriate treatment, which can extent over several weeks or even months. In the past, the mainstay of treatment was based on surgical repair, external drainage of sepsis via chest tubes, and interventional treatment modalities like endoscopic stent deployment or clipping. In 2008, endoscopic vacuum-assisted closure (eVAC) therapy was successfully applied in patients with anastomotic leakages after esophagectomies. As in other vacuum-assisted wound therapies, eVAC cleans the defect by reducing the amount of exudative fluids and necrotic tissue, thus accelerating the healing process by contributing to a better local perfusion as well as through the formation of granulation tissue.”
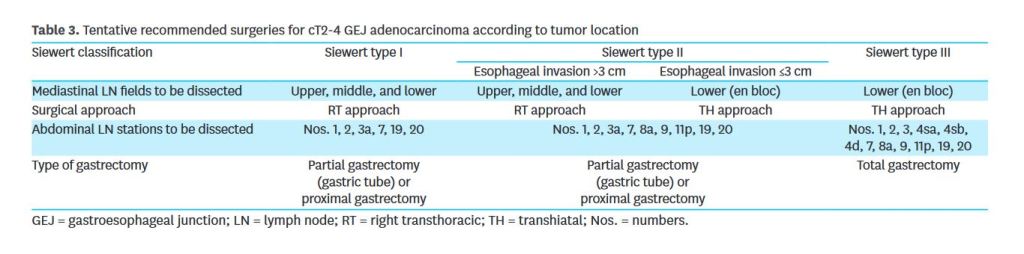
“The Siewert classification is widely used for determining which surgical procedure is used, because previous studies have shown that the pattern of lymph node (LN) metastasis depends on tumor location. In terms of surgical approaches for GEJ adenocarcinoma, a consensus was reached based on two randomized controlled trials. Siewert types I and III are treated as esophageal cancer and gastric cancer, respectively.”
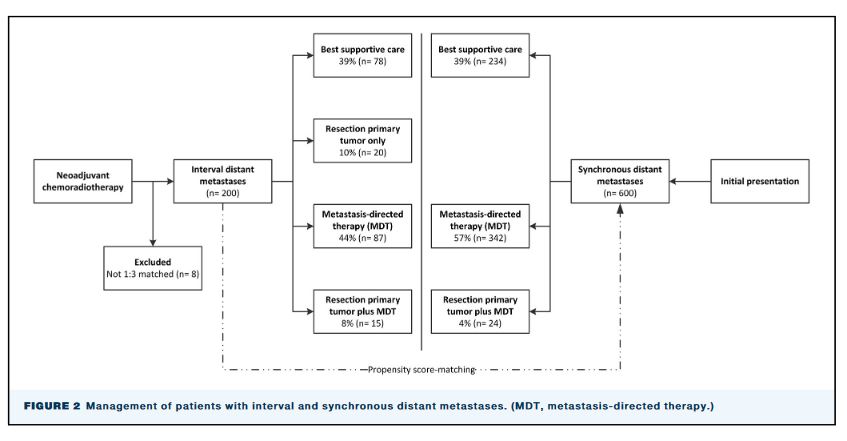
“Neoadjuvant chemoradiotherapy (nCRT) followed by surgery is currently considered an important multimodality treatment option for patients with locally advanced esophageal or gastroesophageal junction cancer. Perioperative chemotherapy is an alternative multimodality treatment option for locally advanced gastroesophageal junction adenocarcinoma. The overall survival of patients with locally advanced esophageal or gastroesophageal junction cancer treated with nCRT followed by surgery remains relatively poor with an estimated 5-year OS rate of 40% to 50%, predominantly due to distant recurrences.”
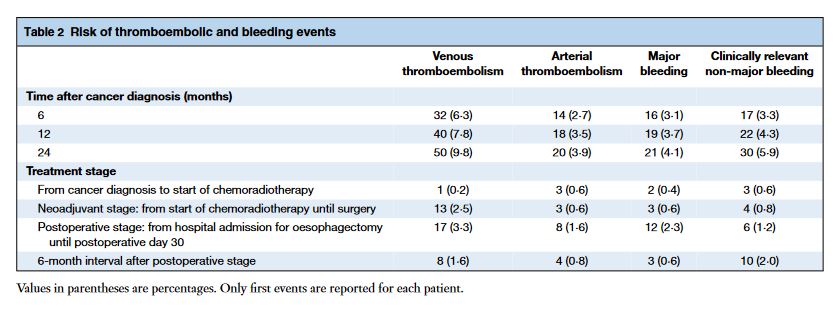
“Patients with oesophageal cancer undergoing neoadjuvant chemoradiotherapy and surgery are at substantial risk of thromboembolic and bleeding events throughout all stages of treatment. Survival is worse in patients with thromboembolic events during follow-up.”