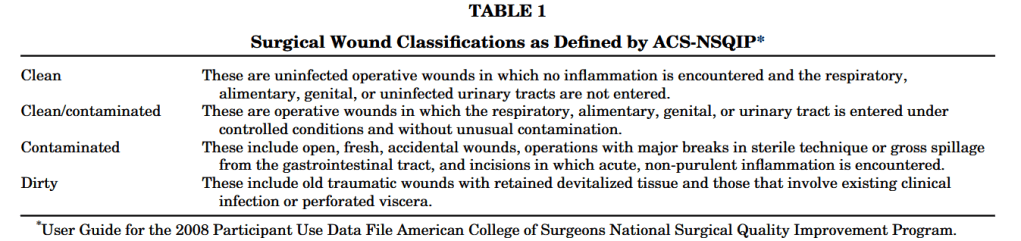
“The wound classification system is an important predictor of postoperative outcomes. Recent studies have focused on elements such as preoperative risk factors and co-morbidities, operative time, prophylactic antibiotic use, and the American Society of Anesthesiology (ASA) physical status score, along with wound classification to predict postoperative surgical outcomes”
“Surgical site infection (SSI) is one of the most common complications following open colon and rectal surgery. Significant morbidity—secondary to increased length of stay, delay in adjuvant treatments, and psychosocial effects—has been well established in the literature. Further, SSIs confer additional monetary costs to the healthcare system.6 Despite best practice recommendations including prophylactic antibiotics and aseptic technique, SSIs remain common in open colorectal surgery. Rates of SSI in the literature range between 15 and 30%. Increased use of laparoscopy in colorectal surgery has significantly impacted rates of SSI but the uptake of laparoscopy has not been complete as certain patients are not candidates and conversion to open is required in approximately 15% of cases.”
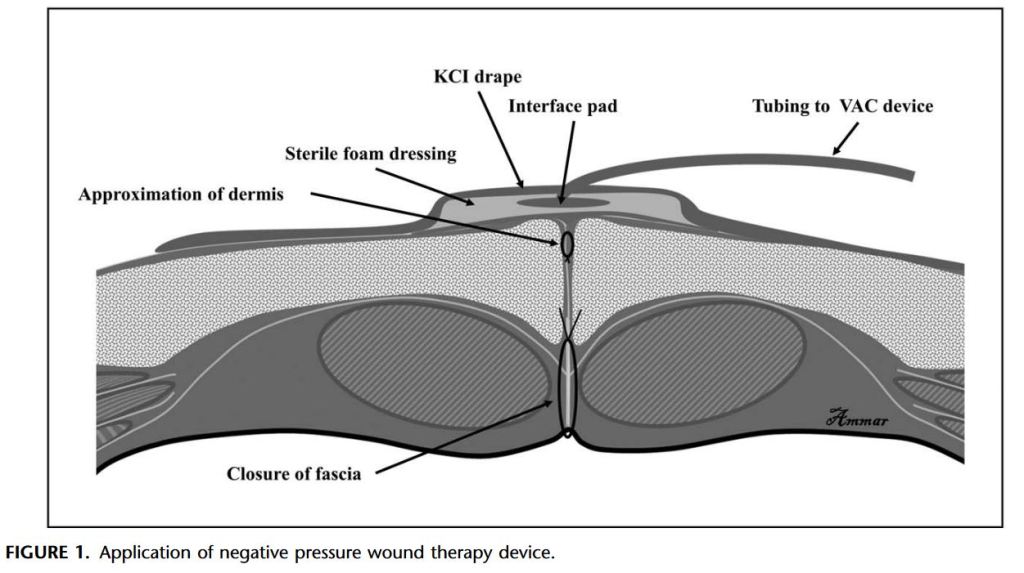
“Despite improvement in infection control, SSIs remain a common cause of morbidity after abdominal surgery. SSI has been associated with an increased risk of reoperation, prolonged hospitalization, readmission, and higher costs. Recent retrospective studies have suggested that the use of negative pressure wound therapy can potentially prevent this complication.”
‘Clostridium perfringens is one of the most widely dispersed opportunistic pathogens and is well known to produce a number of toxins to cause several forms of histotoxic and enteric diseases in humans and animals [2]. Based on the production of four major toxins i.e., alpha, beta, epsilon and iota, it is categorized into five toxin-types viz. A, B, C, D and E. While it is ambiguous why C. perfringens produces so many diverse toxins, it is well known that it uses chromosomally-encoded α-toxin (which has phospholipase C (plc) and sphingomyelinase activities with hemolytic, necrotic and lethal abilities) as a chief virulent factor and key mediator for most of C. perfringens-associated diseases.”
Standard curves representing the quantitative detection of reference strains of C. perfringens by Amp-qPCR assay. C. perfringens ATCC 13124T, ATCC 9856, ATCC 3624, ATCC 3626, ATCC 12917, ATCC 14809, ATCC 27324, and CS 052–1 were cultivated separately in Glu-mGAM. DNA fractions were extracted from the culture samples in the early stationary phase (24 h), and bacterial counts were determined microscopically with DAPI staining. 10-fold serial dilutions of DNA corresponding to the bacterial counts ranging from 100 to 105 bacterial cells were assessed by 16S rRNA gene-specific a, plc-specific b, and cpe-specific c Amp-qPCR assays. The Cq values obtained were plotted against the log10number of bacterial cells subjected to each reaction. Data are expressed as means and standard deviations of the results from 7 strains (ATCC 13124T, ATCC 9856, ATCC 3624, ATCC 3626, ATCC 12917, ATCC 14809, and ATCC 27324) in the 16S rRNA gene-specific and plc-specific primer sets, and 3 strains (ATCC 12917, ATCC 14809, and CS 052–1) in the cpe-specific primer set
There is higher risk of BT in trauma patients, and it is associated with a significant increase of postoperative infections. An abdominal trauma index ≥10 was found to be associated with the development of BT. This is the first study describing BT among patients with abdominal trauma, where causality is confirmed at molecular level.
“Surgical site infections after gastrointestinal perforation with peritonitis have significant morbidity, increased hospital stays, and cost of treatment. The appropriate management of these wounds is still debatable.”
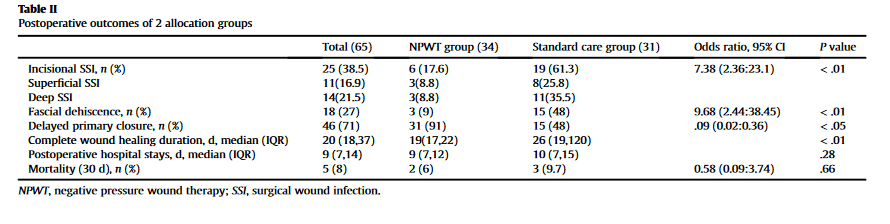
“In this single-center randomized controlled trial, we found that the use of NPWT on the surgical incision in patients with GIP significantly reduced the rate of SSI and wound dehiscence. The overall incidence of SSI in the present study was 38.5%. The use of NPWT also significantly increased the rate of delayed primary wound closure and improved wound healing time.”
“Mesh properties and position within the abdominal wall are the primary determinants in the ability to salvage mesh in the event of PMI. Mesh placed in an intraperitoneal position is rarely salvageable. Similarly, microporous, multifilament, and composite mesh constructs required complete mesh removal in most cases. However, macroporous, monofilament PP mesh in an extraperitoneal position can be salvaged in 72.2% of cases, positively impacting both the need for reoperation for mesh removal and subsequent hernia recurrence.” (Warren)