EUH SURGERY B/EUHM/ ESJH GENERAL SURGERY
Reply

| TOPIC | ARTICLES |
| Portal HTN | Millikan WJ Jr, et al. The Emory prospective randomized trial: selective versus nonselective shunt to control variceal bleeding. Ten year follow-up. Ann Surg. 1985 Jun;201(6):712-22. doi: 10.1097/00000658-198506000-00007. PMID: 3890781; PMCID: PMC1250801. Salam AA, et al. Hemodynamic contrasts between selective and total portal-systemic decompression. Ann Surg. 1971 May;173(5):827-44. doi: 10.1097/00000658-197105000-00022. PMID: 4933303; PMCID: PMC1397510. Wong M, Busuttil RW. Surgery in Patients with Portal Hypertension. Clin Liver Dis. 2019 Nov;23(4):755-780. doi: 10.1016/j.cld.2019.07.003. PMID: 31563221. |
| Non-HPB Cirrhosis General Surgery | Endale Simegn A, et al. Perioperative management of patients with liver disease for non-hepatic surgery: A systematic review. Ann Med Surg (Lond). 2022 Feb 24;75:103397. doi: 10.1016/j.amsu.2022.103397. PMID: 35242334; PMCID: PMC8886011. Johnson KM, et al. Incidence and Risk Factors of Postoperative Mortality and Morbidity After Elective Versus Emergent Abdominal Surgery in a National Sample of 8193 Patients With Cirrhosis. Ann Surg. 2021 Oct 1;274(4):e345-e354. doi: 10.1097/SLA.0000000000003674. PMID: 31714310. Neeff HP, et al. Early mortality and long-term survival after abdominal surgery in patients with liver cirrhosis. Surgery. 2014 Apr;155(4):623-32. doi: 10.1016/j.surg.2013.11.009. PMID: 24468037. Theruvath TP, Adams DB. Preoperative transjugular intrahepatic portosystemic shunt for extrahepatic surgery in cirrhosis. Am Surg. 2010 Jan;76(1):115-7. PMID: 20135955. |
| ECF & Surgical Nutrition | Boullata JI, et al. ASPEN Safe Practices for Enteral Nutrition Therapy [Formula: see text]. JPEN J Parenter Enteral Nutr. 2017 Jan;41(1):15-103. doi: 10.1177/0148607116673053. PMID: 27815525. Compher C, et al. Guidelines for the provision of nutrition support therapy in the adult critically ill patient: The American Society for Parenteral and Enteral Nutrition. JPEN J Parenter Enteral Nutr. 2022 Jan;46(1):12-41. doi: 10.1002/jpen.2267. Erratum in: JPEN J Parenter Enteral Nutr. 2022 Jun 19;: PMID: 34784064. Owen RM, Love TP, Perez SD, Srinivasan JK, Sharma J, Pollock JD, Haack CI, Sweeney JF, Galloway JR. Definitive surgical treatment of enterocutaneous fistula: outcomes of a 23-year experience. JAMA Surg. 2013 Feb;148(2):118-26. doi: 10.1001/2013.jamasurg.153. PMID: 23560282 |
| Inflammatory Bowel Disease | Ban KA, et al. Effect of Diagnosis on Outcomes in the Setting of Enhanced Recovery Protocols. Dis Colon Rectum. 2018 Jul;61(7):847-853. doi: 10.1097/DCR.0000000000001102. PMID: 29878952. Braga Neto MB, et al. Impact of Bariatric Surgery on the Long-term Disease Course of Inflammatory Bowel Disease. Inflamm Bowel Dis. 2020 Jun 18;26(7):1089-1097. doi: 10.1093/ibd/izz236. PMID: 31613968; PMCID: PMC7534455. Hanauer SB, et al.; ACCENT I Study Group. Maintenance infliximab for Crohn’s disease: the ACCENT I randomised trial. Lancet. 2002 May 4;359(9317):1541-9. doi: 10.1016/S0140-6736(02)08512-4. PMID: 12047962. Lowe SC, et al. Declining Rates of Surgery for Inflammatory Bowel Disease in the Era of Biologic Therapy. J Gastrointest Surg. 2021 Jan;25(1):211-219. doi: 10.1007/s11605-020-04832-y. PMID: 33140318. Kline BP, et al. Clinical and Genetic Factors Impact Time to Surgical Recurrence After Ileocolectomy for Crohn’s Disease. Ann Surg. 2021 Aug 1;274(2):346-351. doi: 10.1097/SLA.0000000000003660. PMID: 31714311. Myrelid P, Kalman TD. Old, New, and Out of the Box in IBD Surgery: Proceedings of the European Crohn’s and Colitis Organisation 2020 Congress from a Surgical Perspective. Dis Colon Rectum. 2021 Aug 1;64(8):929-931. doi: 10.1097/DCR.0000000000002102. PMID: 33872289 Reinisch W, et al. Long-term infliximab maintenance therapy for ulcerative colitis: the ACT-1 and -2 extension studies. Inflamm Bowel Dis. 2012 Feb;18(2):201-11. doi: 10.1002/ibd.21697. PMID: 21484965. |
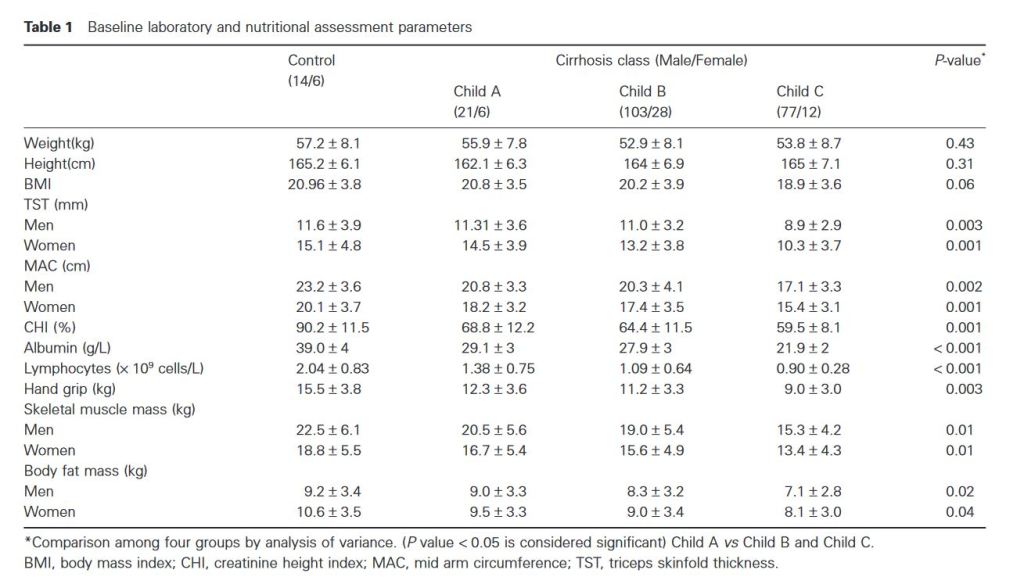
“Prevalence of malnutrition in chronic liver disease ranges between 10% and 100%, depends on severity of liver disease. Prevalence is more in patients with alcoholic cirrhosis compared to nonalcoholic cirrhotics. 3 Malnutrition is seen in all clinical stages but is easier to detect in advanced stages of liver cirrhosis. Many patients have subtle changes such as fat soluble vitamin deficiency, anemia from iron, folate or pyridoxine deficiency, altered cell-mediated immune functions and minimal loss of muscle mass, while patients with end-stage liver disease have muscle wasting, decreased fat stores, and cachexia.”
“Complications are known to occur at each and every step of hernia surgery. Applying caution while performing each step can save the patient from a lot of morbidity. One starts by applying strict patient selection criteria for endoscopic hernia repair, especially in the initial part of ones learning curve. A thorough knowledge of anatomy goes a long way in avoiding most of the complications seen in hernia repair. This anatomy needs to be relearned from what one is used to, as the approach is totally different from an open hernia repair. And finally, learning and mastering the right technique is an essential prerequisite before one ventures into inguinal hernia repair.”
“The most important preoperative precaution is proper patient selection prior to surgery, especially in the initial part of the learning curve. Ideally, direct or small indirect hernias are best. Large hernias, obese patients and irreducible, obstructed hernias are best avoided. An absolute contraindication is strangulated hernia. Also a detailed work-up of elderly patients to assess cardiorespiratory status is mandatory to ensure a safe outcome.”
Continue reading“Management of blunt spleen injuries has evolved from mandatory splenectomy to non-operative management (NOM) allowing for splenic salvage. The Eastern Association for the Surgery of Trauma (EAST) practice management guideline for the management of blunt solid organ injury recommends NOM in splenic injury regardless of age, grade, or associated injuries.”
“Splenectomy continues to be the treatment of choice in patients with unstable hemodynamics and a known splenic injury. In the hemodynamically normal patient, current practice is to observe the patient and treat with NOM to save the patients the complications associated with surgery.”
Continue reading“Growing evidence suggests an increasing significance for the extent of gastrointestinal tract (GIT) dysfunction in Parkinson’s disease (PD). Most patients suffer from GIT symptoms, including dysphagia, sialorrhea, bloating, nausea, vomiting, gastroparesis, and constipation during the disease course. The underlying pathomechanisms of this α-synucleinopathy play an important role in disease development and progression, i.e., early accumulation of Lewy pathology in the enteric and central nervous systems is implicated in pharyngeal discoordination, esophageal and gastric motility/peristalsis impairment, chronic pain, altered intestinal permeability and autonomic dysfunction of the colon, with subsequent constipation.”

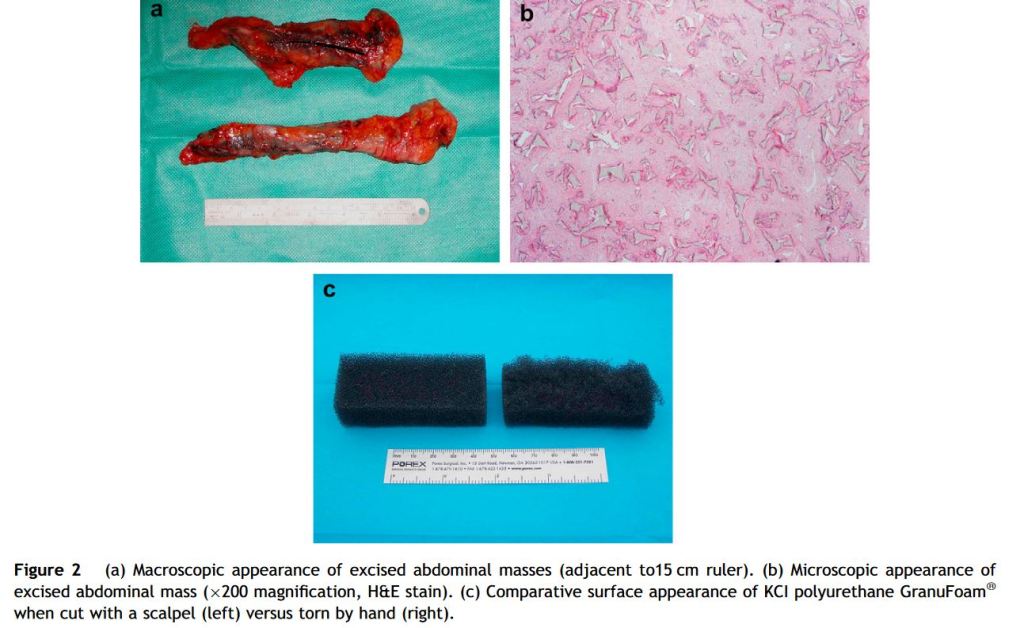
With large cavitating wounds, there is a risk of sponge retention that may be all too easily
overlooked, particularly with the surgeons’ habit of cutting the sponge to the desired shape and the use of multiple fragments. We therefore recommend that a count is made of the number of sponges used – as is standard practise for swabs, needles and instruments.