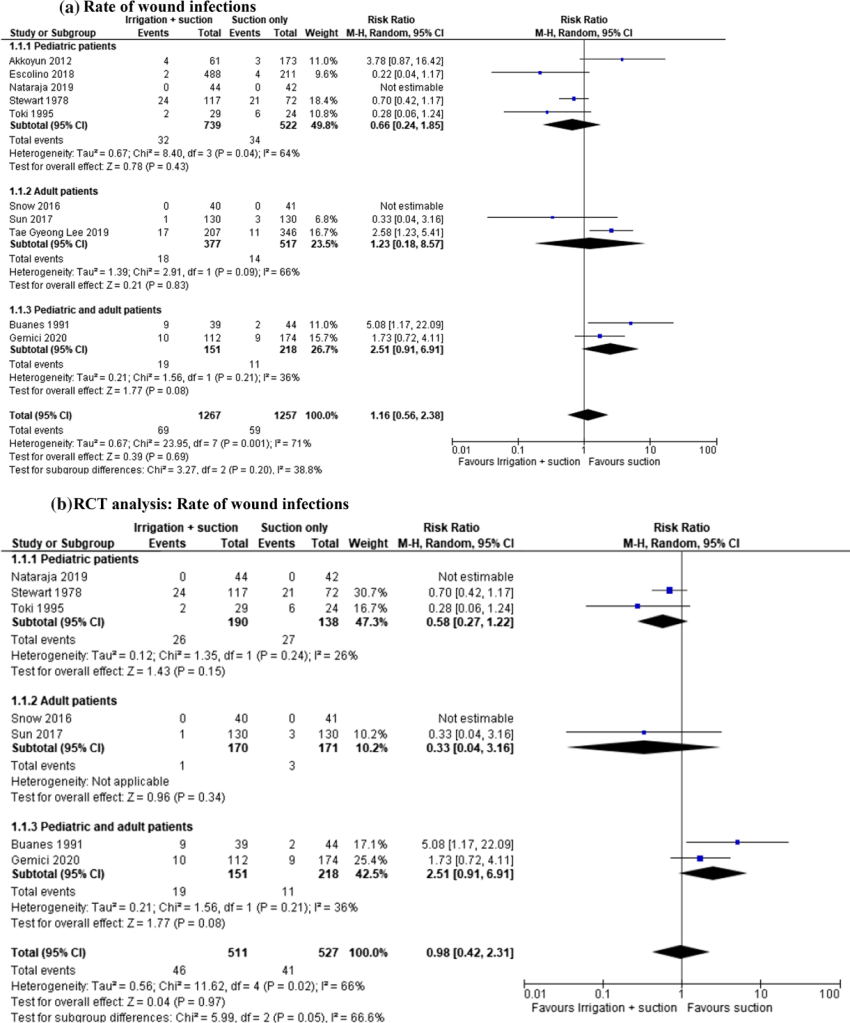
“The management of IAA remains controversial with different strategies suggested to decrease its incidence: antibiotic prophylaxis, post-operative antibiotic therapy, peritoneal irrigation with saline solution or suction only of the abscess/purulent liquid without irrigation of the cavity during appendectomy. In the literature, many studies address this topic; however, currently there is no evidence to clearly demonstrate the effectiveness of peritoneal irrigation over suction only. Italian guidelines recommend thorough peritoneal lavage (6–8 L of warm saline) and aspiration to minimize the IAA rate in complicated appendicitis. The recent WSES (World Society of Emergency Surgery) guidelines report that “Peritoneal irrigation does not have any advantage over suction alone in complicated appendicitis in both adults and children. The performance of irrigation during laparoscopic appendectomy does not seem to prevent the development of IAA and wound infections
in neither adults nor paediatric patients”. WSES recommendation is “to perform suction only in complicated appendicitis patients with intra-abdominal collections undergoing laparoscopic appendectomy” [QoE: Moderate; Strength of recommendation: Strong; 1B]). The concern regarding irrigation and lavage is that these procedures might help spread the infectious material.”