One discussion this week focused on complications after neck dissections.
Reference: Man LX, Beswick DM, Johnson JT. Antibiotic prophylaxis in uncontaminated neck dissection. Laryngoscope. 2011 Jul;121(7):1473-1477. doi:10.1002/lary.21815.
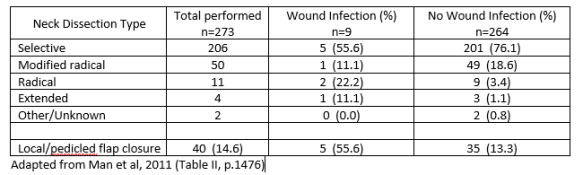
Summary: Man et al (2011) performed a retrospective chart review of 273 uncontaminated neck dissections in order to identify risk factors for postoperative wound infections and to describe the outcomes of antibiotic prophylaxis use. Only 15%
Wound infection was not associated with age, sex, tobacco and alcohol use, history of head/neck surgery, history of radiation/chemotherapy, or number of drains placed during surgery.
Wound infection was independently associated with longer operative time, local/pedicled flap closure and radical or extended neck dissection (p.1474).
Their results for risk of wound infection by type of dissection are below. All 9 wound infections occurred in those receiving intraoperative antibiotics only (4) or intra- and postoperative antiobiotics (5).
Additionally, this study found that antibiotics are prescribed more frequently to older patients, possibly because they are perceived as less healthy (p.1475). Patients requiring more extensive operations are at a higher risk of postoperative infection, as are those who undergo an operation involving the re-positioning of the patient’s head thus exposing the surgical field (p.1476). The under-reporting of postoperative complications in outpatient settings may also contribute to an underestimate of wound infection.
This review was not able to confirm or support the use of antibiotic prophylaxis in uncontaminated neck dissection significantly lowers the risk of infection. Still, the authors recommend its use “for more extensive lymphadenectomy procedures including radical neck dissection, extended neck dissection, or those requiring longer operative time” (p.1477).