“Neoadjuvant chemoradiotherapy followed by surgery is currently considered an important multimodality treatment option for patients with locally advanced esophageal or gastroesophageal junction cancer. Perioperative chemotherapy is an alternative multimodality treatment option for locally advanced gastroesophageal junction adenocarcinoma.”
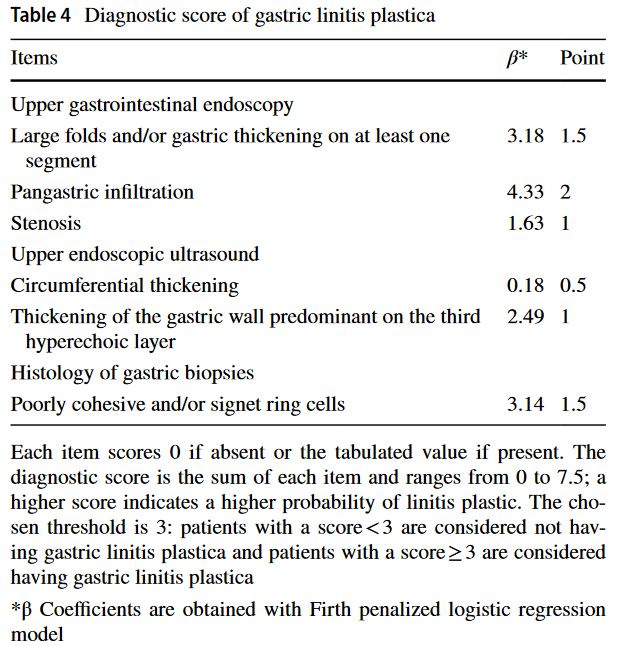
“In this retrospective study, all patients who had gastrectomy for cancer between 2007 and 2017 in French tertiary centers were included. The outcome was a diagnosis of GLP based on pathological review of the surgical specimen. The diagnostic score was created by using variables that were most frequently associated with GLP using penalized logistic regression on multiply imputed datasets. We used discrimination measures to assess the performances of the score. Internal validation was performed using bootstrapping methods to correct for over-optimism.”
“The diagnosis of LP carries significant controversy regarding its surgical management. Lymph node involvement is almost always present at the time of diagnosis, and due to its diffuse nature, microscopic disease is often found at the resection margins. Peritoneal dissemination is frequently encountered at the time of surgery or as the main site of recurrence. As such, curative resection is possible in less than half of patients and early recurrence is common, leading to a dismal median survival, ranging from 6 to 12 months, and 5-year survival between 8 and 13 %.”
“Linitis plastica (LP) is a distinct phenotype of gastric cancer. Macroscopically, it is characterized as a thickened stomach, with prominent diffusion of the tumor into the submucosal and muscular layers; microscopically, it is often associated with signet ring cell features and diffuse and scirrhous (referring to the histologic characteristic of abundant stromal cells) histologic types.”
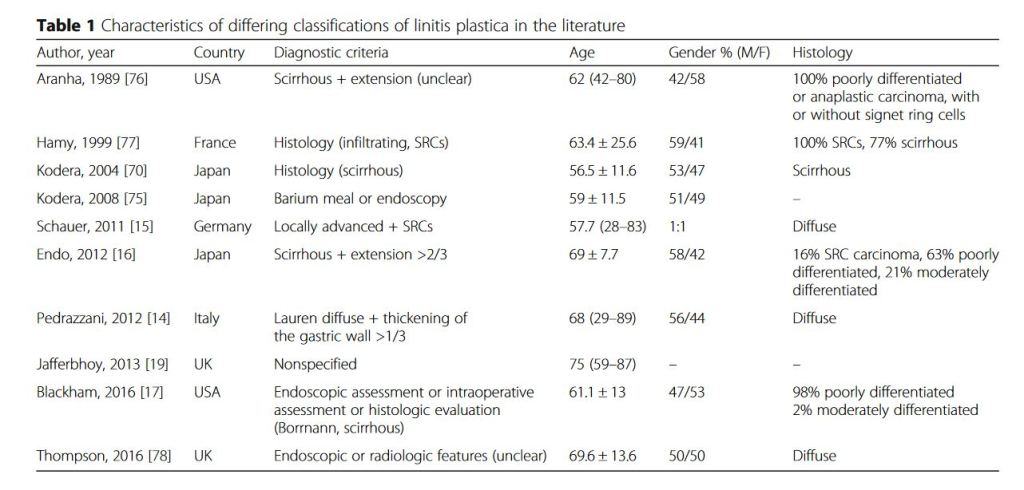
“Linitis plastica due to gastric adenocarcinoma is a condition with a long history, but still lacks a standardized definition and is commonly confused with Borrmann type IV, Lauren diffuse, and signet-cell type gastric cancer. The absence of a clear definition is a problem when investigating its biological characteristics and role as a possible independent factor for prognosis. Nevertheless, the biological behavior for linitis plastica, which is unique, may be valuable in risk stratification and have implications for treatment. A definition of linitis plastica based on molecular or genomic criteria could represent a useful starting point for investigating new targeted therapies.”
“Gastric acid production is necessary for the body to digest food and break down nutritional components into absorbable amino acids, carbohydrates, and fats. Most of the acid is produced when gastric pH stimulates the release of gastrointestinal using the release and activation of various digestive enzymes. The stomach is a relatively acidic environment with a pH of less than 4.0, which can drop to 2.0 with parietal cells. Parietal cells live in the fundus and the body of the stomach and secrete hydrogen ions. This activity explains when this condition should be considered on a differential diagnosis, articulates how to properly evaluate for this condition, and highlights the role of the interprofessional team in caring for patients with this condition.”
Early use of PPIs and H2 blockers in patients can be beneficial to prevent stress gastritis.
PPIs work to inhibit hydrogen ion secretion by blocking the H/K ATPase of parietal cells.
Parietal cells are stimulated by acetylcholine, gastrin, and histamine to secrete hydrogen ions.
Acetylcholine and gastrin via phospholipase and PKC to stimulate hydrogen ion secretion.
Histamine works through cAMP and PKA to stimulate hydrogen ion secretion.
The most common presenting symptom is bleeding (bloody nasogastric tube, melena).
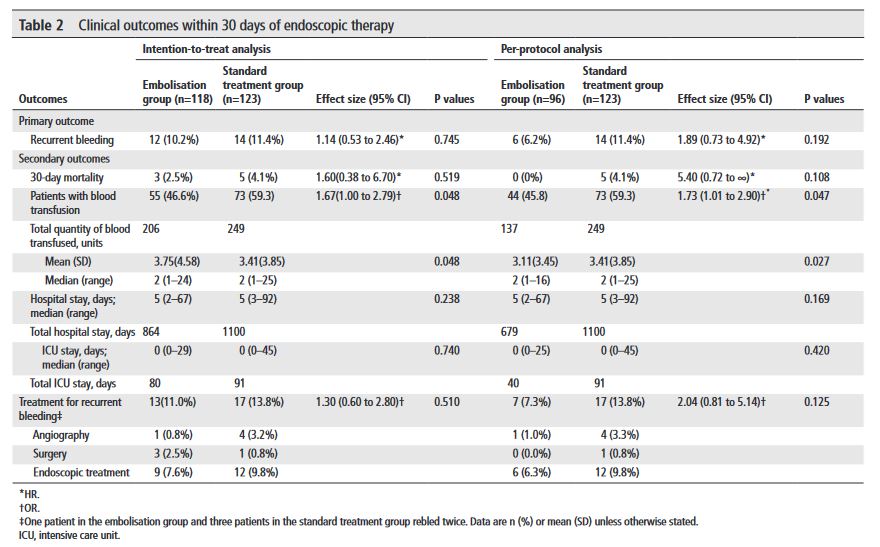
“Acute upper gastrointestinal bleeding (AUGIB) is one of the most common emergencies in gastroenterology. Despite major improvements in its management, AUGIB continues to be associated with significant morbidity and mortality. Bleeding peptic ulcers are one of the principal causes of AUGIB. Endoscopic therapy to bleeding ulcers reduces further bleeding and improves patients’ outcomes”