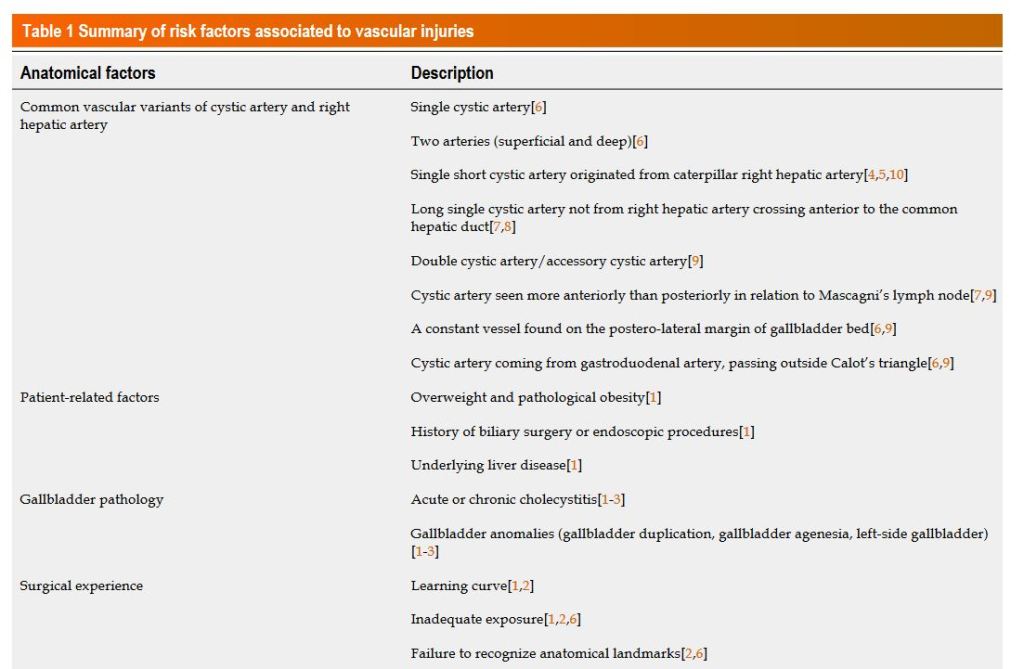
“Several risk factors may contribute to vascular injuries during laparoscopic cholecystectomy: Anatomical factors, including vascular anomalies, patient-related factors, the gallbladder pathology and surgeon’s experience. Concerning the anatomical factors, the different variants of vascular anatomy may represent a possible cause of bile duct injuries, particularly anomalies of the cystic artery and right hepatic artery (RHA). If surgeons are not aware of possible variations of the RHA, such as in the case of acute and chronic cholecystitis with unclear anatomy of Calot’s triangle, the RHA may be accidentally injured or mistaken for the cystic artery and actively cut off”
“Parastomal hernia, defined as an incisional hernia at the abdominal wall defect resulting from stoma formation, is a frequent complication of enterostomy (ileostomy and jejunostomy), colostomy, and urostomy. A growing body of evidence supports the use of prophylactic mesh at the time of stoma creation to prevent the development of PSH. In particular, the use of permanent mesh has been supported in the creation of an end colostomy, and prophylactic mesh has been studied for use in other types of stoma.”
“Hiatus hernia contributes to the pathophysiology of gastroesophageal reflux disease (GERD). Mesh-augmentation of surgical repair might be associated with a reduced risk of recurrence and GERD. However, recurrence rates, mesh-associated complications and quality of life after mesh versus suture repair are debated. The aim of this meta-analysis was to determine HH recurrence following mesh-augmentation versus suture repair.”
“Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), affects ~10 million people worldwide every year, representing the third most common cardiovascular disease globally. The 30-day case fatality rate after VTE diagnosis is 10.6%, with about 30% to 50% of survivors developing long-term complications that increase the burden of this disease.”
“An increased risk of DVT and PE in patients with IBD has been evident for the past 75 years. Most work in this area has not looked specifically at patients undergoing surgery. Patients with IBD frequently require surgical intervention, and an understanding of their risk of venous thromboembolism is therefore an important issue. This study aimed to examine rates of DVT and PE in patients with IBD undergoing surgery using data from the NSQIP.”
‘Clostridium perfringens is one of the most widely dispersed opportunistic pathogens and is well known to produce a number of toxins to cause several forms of histotoxic and enteric diseases in humans and animals [2]. Based on the production of four major toxins i.e., alpha, beta, epsilon and iota, it is categorized into five toxin-types viz. A, B, C, D and E. While it is ambiguous why C. perfringens produces so many diverse toxins, it is well known that it uses chromosomally-encoded α-toxin (which has phospholipase C (plc) and sphingomyelinase activities with hemolytic, necrotic and lethal abilities) as a chief virulent factor and key mediator for most of C. perfringens-associated diseases.”
Standard curves representing the quantitative detection of reference strains of C. perfringens by Amp-qPCR assay. C. perfringens ATCC 13124T, ATCC 9856, ATCC 3624, ATCC 3626, ATCC 12917, ATCC 14809, ATCC 27324, and CS 052–1 were cultivated separately in Glu-mGAM. DNA fractions were extracted from the culture samples in the early stationary phase (24 h), and bacterial counts were determined microscopically with DAPI staining. 10-fold serial dilutions of DNA corresponding to the bacterial counts ranging from 100 to 105 bacterial cells were assessed by 16S rRNA gene-specific a, plc-specific b, and cpe-specific c Amp-qPCR assays. The Cq values obtained were plotted against the log10number of bacterial cells subjected to each reaction. Data are expressed as means and standard deviations of the results from 7 strains (ATCC 13124T, ATCC 9856, ATCC 3624, ATCC 3626, ATCC 12917, ATCC 14809, and ATCC 27324) in the 16S rRNA gene-specific and plc-specific primer sets, and 3 strains (ATCC 12917, ATCC 14809, and CS 052–1) in the cpe-specific primer set
‘The term ‘bacterial translocation’ is used to describe the passage of viable resident bacteria from the gastrointestinal tract to normally sterile tissues such as the mesenteric lymph nodes and other internal organs.7 The term also applies to the passage of inert particles and other macromolecules, such as lipopolysaccharide endotoxin, across the intestinal mucosal barrier.’
‘Bacterial translocation has been shown to occur in various patient populations.6 As already stated, it occurs in patients undergoing elective abdominal surgery, organ donors and those with intestinal obstruction, colorectal cancer, ischaemia–reperfusion injury shock and pancreatitis. Many authors suggest an increased prevalence in patients with obstructive jaundice, those receiving parenteral nutrition and the malnourished, but the evidence for this is limited. Interestingly, translocation, assessed by endotoxin or bacterial culture of portal or systemic blood, has only rarely been demonstrated after trauma’