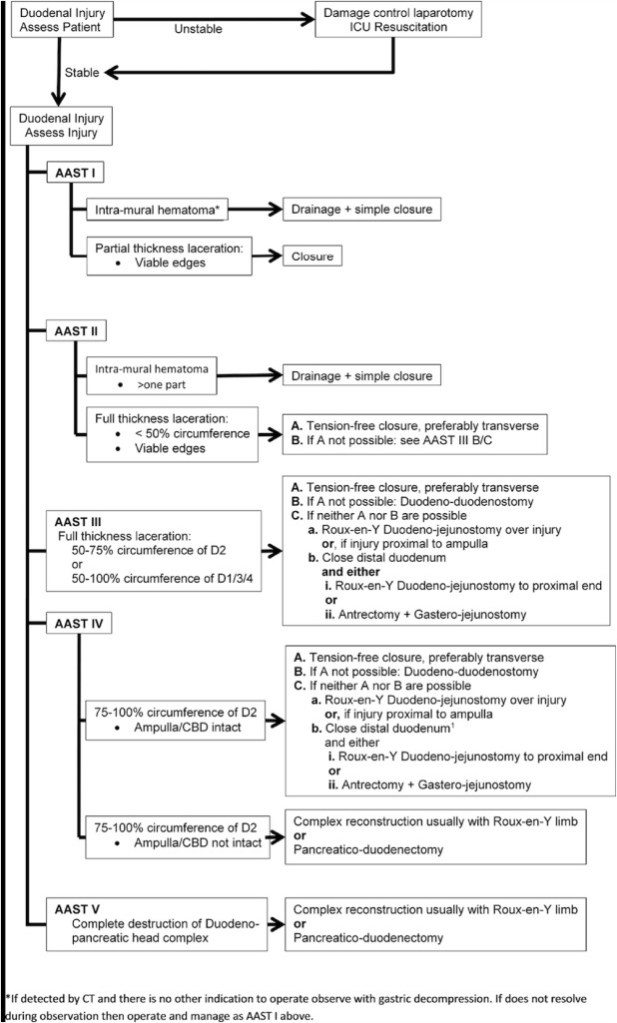
“Duodenal trauma is a rare occurrence existing in 1–4.7% of all abdominal trauma. Its posterior and partially retroperitoneal location shields it from most traumatic mechanisms. Colloquially referred to as the ‘surgical soul’, its proximity to complex regional anatomy makes duodenal trauma particularly at risk for biliary, pancreatic and major vascular injury with 68–86.5% of patients sustaining an associated injury.”
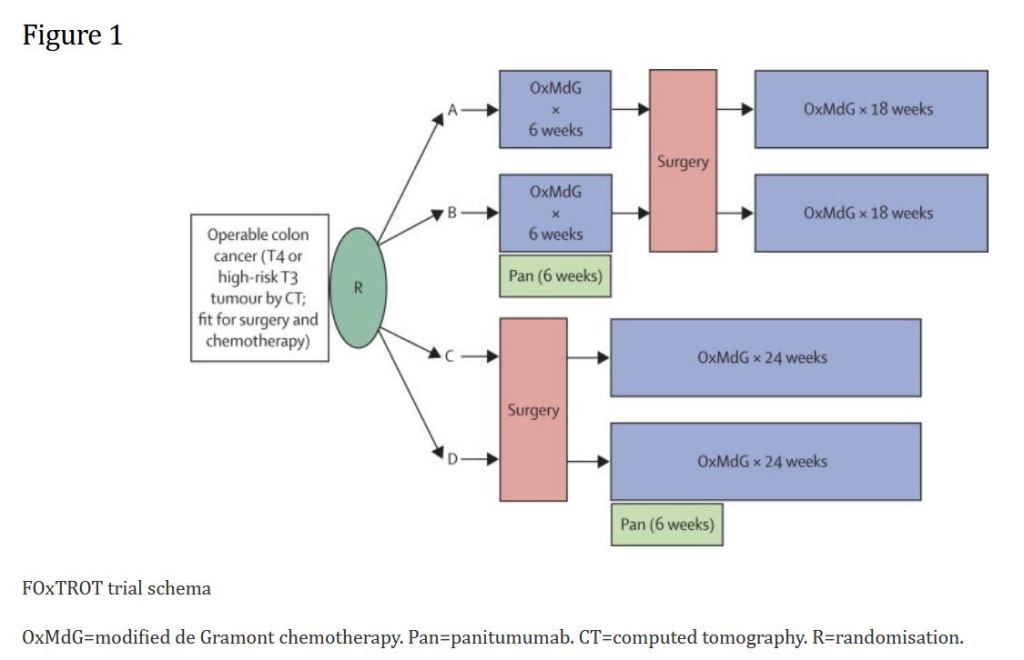
“Preoperative (neoadjuvant) chemotherapy and radiotherapy are substantially more effective than similar postoperative therapy in oesophageal, gastric, and rectal cancer. Earlier treatment might be more effective at eradicating micrometastatic disease than the same treatment 3 months later, the typical period between diagnosis and starting postoperative chemotherapy, particularly because surgery increases growth factor activity in the early postoperative period, promoting more rapid tumour progression.”
“The overall incidence of duodenal injuries in severely injured trauma patients is between 0.2 to 0.6% and the overall prevalence in those suffering from abdominal trauma is 3 to 5% 1,2. Approximately 80% of these cases are secondary to penetrating trauma, commonly associated with vascular and adjacent organ injuries. These associated injuries create a significant challenge towards the early diagnosis and appropriate management. Therefore, defining the best surgical treatment algorithm remains controversial. Mild to moderate duodenal trauma is currently manage via primary repair and simple surgical techniques. However, severe injuries have required complex surgical techniques (duodenal diverticulization, pyloric exclusion with or without gastrojejunostomy and pancreatoduodenectomy) without significant favorable outcomes and consequential increase in the rates of mortality.”