“Right hemicolectomy is considered one of the simplest colorectal major procedures and is often considered an appropriate first step for residents and young fellows. Despite this, complications after right hemicolectomy for cancer are common, at ≈30%, and postoperative mortality is reported to be ≈3%. Anastomotic leak (AL) after right hemicolectomy for cancer is a major contributor to this short-term morbidity and mortality. The document AL rate after right hemicolectomy ranges widely, from 1.3% to 8.4%. This also has a significant impact on healthcare costs and major oncologic consequences, as demonstrated by the higher cancer recurrence rate after AL.”
“Colorectal cancer is the second-leading cause of cancer-related mortality in both the United States and Europe. With respect to prognosis, increasing evidence has suggested that systemic inflammation is a key predictor of disease progression and survival for colorectal cancer patients undergoing surgery. Furthermore, whereas red blood cell (RBC) transfusions may be life-saving in some circumstances, there has been growing evidence that transfusions are associated with adverse postoperative outcomes, including infectious complications and cancer recurrence. These detrimental effects are thought to be related to systemic inflammation and transfusion-related immunomodulation (TRIM). Whereas the exact mechanisms remain unknown, TRIM seems to be related to various immunologic changes, including decreased interleukin (IL)-2 production, monocyte and cytotoxic cell activity inhibition, increased suppressor T-cell activity, and immunosuppressive prostaglandin release.”
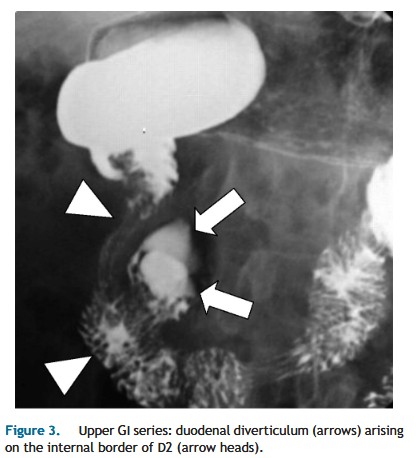
“Despite their frequent occurrence, DD are asymptomatic in 95% of cases, while 1 to 5% eventually become symptomatic. Intervention is indicated only for symptomatic duodenal diverticula(DD). Complications related to DD are rare but may be very severe; they include biliary or pancreatic obstruction, duodenal obstruction, perforation, or hemorrhage. Endoscopic treatment is usually the first-line approach to biliopancreatic complications related to juxtapapillary DD and also for hemorrhagic complications. Indirect surgical treatments include bilio-enteric bypasses and even duodenal exclusion. Direct surgical treatment consists of duodenal diverticulectomy, which has significant morbidity and mortality; prophylactic excision of asymptomatic DD is therefore not recommended.”
“A surgical site infection (SSI) is defined as an infection of the incision (superficial SSI), the tissue below the incision (deep SSI), or within the abdominal cavity (organ space SSI). SSI accounts for more than 20% of all health care-associated infections and is the most common infection after surgery, affecting an estimated 300,000 patients annually. Compared with other surgical subspecialties, patients undergoing colorectal surgery are at the highest risk for developing an SSI with an estimated incidence of 5% to 30%. Patients undergoing emergency colorectal surgery with colon perforation have an SSI incidence as high as 80%.”
TABLE 2.
Summary and strength of GRADE recommendations for preventing SSIs
Summary
Recommendation strength
GRADE quality of evidence
1
Implementing an SSI bundle for patients undergoing colorectal surgery can decrease the incidence of SSI
Strong
Moderate
2
Oral antibiotics in combination with mechanical bowel preparation have been shown to decrease the incidence of SSI after elective colorectal resection
Strong
Moderate
3
In circumstances where a mechanical bowel preparation is contraindicated or otherwise omitted, preoperative oral antibiotic preparation alone can reduce the incidence of SSI
Conditional
Moderate
4
Showering with chlorhexidine before colorectal surgery does not significantly impact SSI rates
Strong
Moderate
5
Smoking cessation before surgery may be recommended to reduce the risk of SSI
Conditional
Moderate
6
On the day of colorectal surgery, patients should have their hair removed from the surgical site using a clipper or not removed at all. Shaving with a razor before surgery is discouraged
Strong
Moderate
7
Patients undergoing colorectal resection should have parenteral antibiotics administered within 60 min of incision. Dosing and redosing should be based on the pharmacokinetic profile of the antibiotic
Strong
Low
8
Patients who report a penicillin allergy may be evaluated for having true hypersensitivity and high-risk reactions to penicillin. Delabeling a penicillin-allergic patient can facilitate the appropriate use of a preoperative prophylactic beta-lactam antibiotic and improve outcomes
Conditional
Low
9
For most clean and clean-contaminated cases, prophylactic parenteral antibiotics should be limited to the initial 24 h postoperatively
Strong
Moderate
10
Cleansing the surgical site with chlorhexidine–alcohol-based preparation is typically recommended for patients undergoing colorectal surgery
Strong
Moderate
11
Hyperglycemia on the day of surgery and in the immediate postoperative period may increase the risk of SSI after elective colorectal resection
Conditional
Moderate
12
Maintaining intraoperative normothermia may decrease the incidence of SSI in patients undergoing colorectal surgery
Conditional
Low
13
High-fractionated oxygen is not routinely recommended to prevent SSI
Conditional
Moderate
14
Wound protectors can decrease the incidence of SSI after colorectal surgery
Strong
High
15
Minimally invasive colorectal surgery can decrease the incidence of SSI compared to open surgery
Strong
High
16
Topical antimicrobial agents applied to the surgical incision are not recommended
Strong
Low
17
NPWT for primarily closed incisions may decrease the incidence of SSI
Conditional
Moderate
18
Advanced silver or antimicrobial dressings are not routinely recommended for clean or clean-contaminated wounds after colorectal surgery
Conditional
Moderate
GRADE = Grading of Recommendations, Assessments, Development, and Evaluation; NPWT = Negative pressure wound therapy; SSI = surgical site infection.
“Higher rates of morbidity and mortality following colonic conduits are reported to be due to be associated with longer operating times and the additional colo-gastric and colo-colic anastomoses. Yet, colonic conduits have the advantages of being longer, acid resistant, and possess an excellent blood supply. No consensus regarding the optimum site of colonic conduit (right vs. left) or placement route (posterior mediastinal, retrosternal or subcutaneous) exists. The operation is usually carried out based on individual surgeons’ preferences and experience, and in the absence of randomised controlled trials, this situation is likely to continue. The aim of this systematic review and meta-analysis was to determine the optimal site of colonic conduit and route of placement after adult oesophagectomy.”
“Small-bowel obstruction (SBO) is responsible for up to 16% of hospital admissions for abdominal pain with mortality ranging between 2% and 8% overall, and as high as 25% when associated with bowel ischemia. Radiologic imaging plays the key role in the diagnosis and management of SBO because neither patient presentation, the clinical examination, nor laboratory testing are sufficiently sensitive or specific enough to diagnose or guide management. Imaging not only diagnoses the presence of SBO but also can aid in the differentiation of high-grade from low-grade obstruction. This differentiation helps to guide referring physicians between surgical treatment for high-grade or complicated SBO versus conservative management with enteric tube decompression.”
“Chronic intestinal failure (CIF) is a rare but feared severe complication of Crohn’s disease, with 60% of patients permanently dependent on parenteral nutrition. This review aims to summarize the knowledge available in the current literature describing recent advances in the management and treatment of adult patients with CIF, with emphasis on patients with Crohn’s disease. Moreover, it aims to further understanding of modern approaches to CIF complications such as catheter-related bloodstream infections and intestinal failure-associated liver disease.”