“Rates of postoperative bleeding and transfusion are either widely variable or often unreported. As a high-volume center, we have anecdotally appreciated significant rates of each but admittedly have not accurately reported the degree of this specific morbidity in our practice. This study aims to quantify postoperative blood loss, rates of blood transfusion, and the incidence of operative or endovascular intervention for bleeding, as well as associated risk factors contributing to this morbidity in patients undergoing open TAR.”
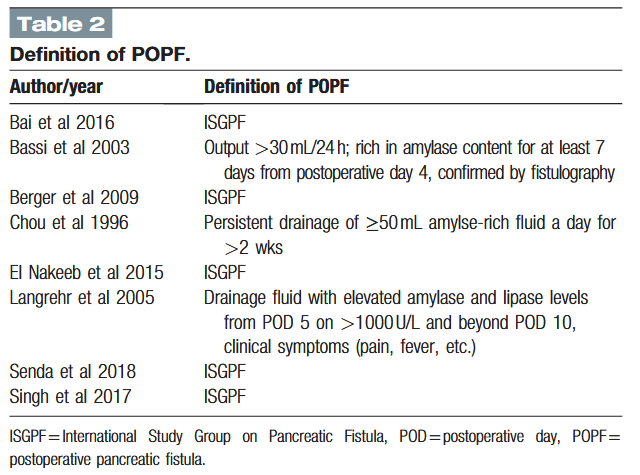
“Pancreaticoduodenectomy (PD) is a complex, high-risk standard surgical procedure that is indicated primarily for periampullary diseases. Central to the entire discipline of PD are postoperative mortality and morbidity. Although operative mortality in patients undergoing PD has decreased, the incidence of postoperative morbidity remains high at 40% to 50%. Postoperative pancreatic fistula (POPF) is the most common complication, with rates ranging from 5% to 30% in previous studies. Many methods have been described to decrease the risk of POPF, including the use of medications (prophylactic octreotide, sealants), prophylactic pancreatic stenting, and improvements in pancreatic reconstruction techniques. The most commonly used pancreatic reconstruction techniques are pancreaticogastrostomy (PG) and pancreaticojejunostomy (PJ).”
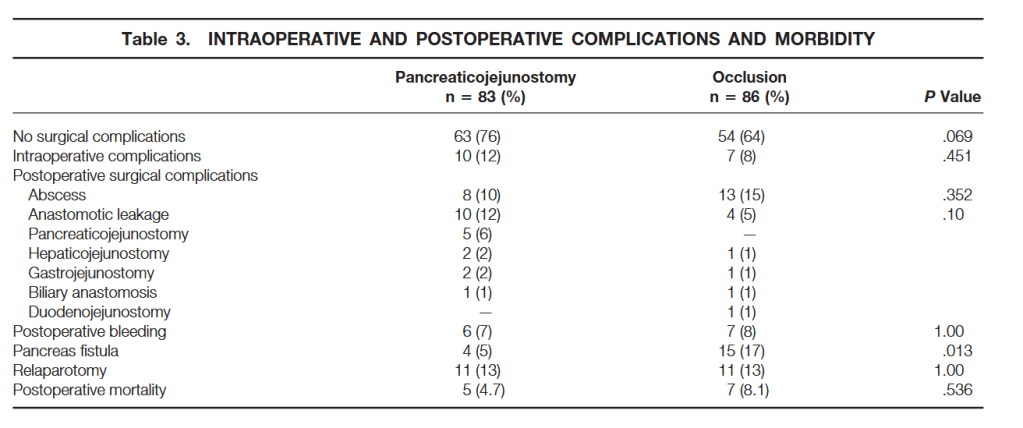
“Pancreatic fistulas and pancreatitis may develop in the pancreatic remnant and may lead to hemorrhage, sepsis, and subsequent death. Procedures to avoid pancreaticojejunostomy were described, including total pancreatectomy. None of these has so far proven to diminish morbidity significantly. Another technique investigated is obliteration closure of the pancreatic duct with a chemical substance, thus avoiding a pancreaticojejunostomy. This method was proposed by Gebhardt et al. They studied the effect of occlusion of the pancreatic duct system with Ethibloc, an alcoholic prolamine, in animal experiments. The pancreatic duct may also be occluded with a fibrin glue solution, Tissucol, which was found to have a more protective effect on beta cell function than the other solutions used.”
“Pancreatoduodenectomy (PD) is the gold standard surgical procedure performed for both benign and malignant diseases of the pancreas and periampullary region. Since the introduction of PD by Whipple in 1941, the treatment of the pancreatic stump was felt as primary issue due to the frequency of the complications. Advances in medical and surgical care have made the mortality rate after PD declined dramatically (0e5%), even in centres with experienced surgeons. However, the morbidity rate remains quite high, approaching the 50%. The most common complications after PD are pancreatic fistula, late gastric empty, haemorrhage, hepatic-jejunostomy leakage, wound infection and intraabdominal abscess, which affect mortality rate, hospitalization and costs. At present, pancreatic fistula (PF) is the most significant complication, with a rate ranges from 5% to 40% even in tertiary centers. About the 40% of the patient deaths are the results of septic and haemorrhagic complication following PF. Although, attempting to reduce complications, many refinements of the cur- rent surgical techniques, pancreatico-jejunostomy, pancreaticogastrostomy and duct occlusion, have been proposed. Nevertheless, the best method to manage the pancreatic stump is still debated.”
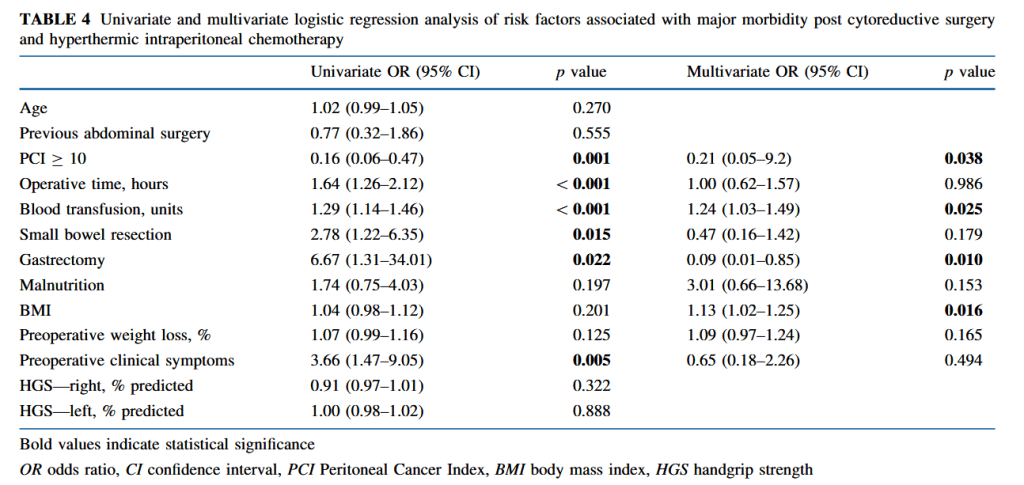
“Cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) is complex surgery to treat peritoneal surface malignancy (PSM). PSM arises from gastrointestinal (GI), gynecological, or primary peritoneal cancers. CRS aims to completely remove macroscopic tumor. In order to achieve complete cytoreduction, multiple abdominal organ resections are often necessary. After cytoreduction, HIPEC is delivered into the abdominal cavity for 30–90 min to treat residual microscopic disease.” “Malnutrition is prevalent in patients undergoing surgery for abdominopelvic malignancy and is associated with increased morbidity, longer hospital length of stay (LOS), and mortality. Preoperative malnutrition is a risk factor for organ dysfunction, impaired immune function, wound complications, impaired physical function, and increased LOS. Malnutrition prevalence is documented in up to 67% of patients with ovarian cancer and 30–50% of patients with colorectal cancer.”
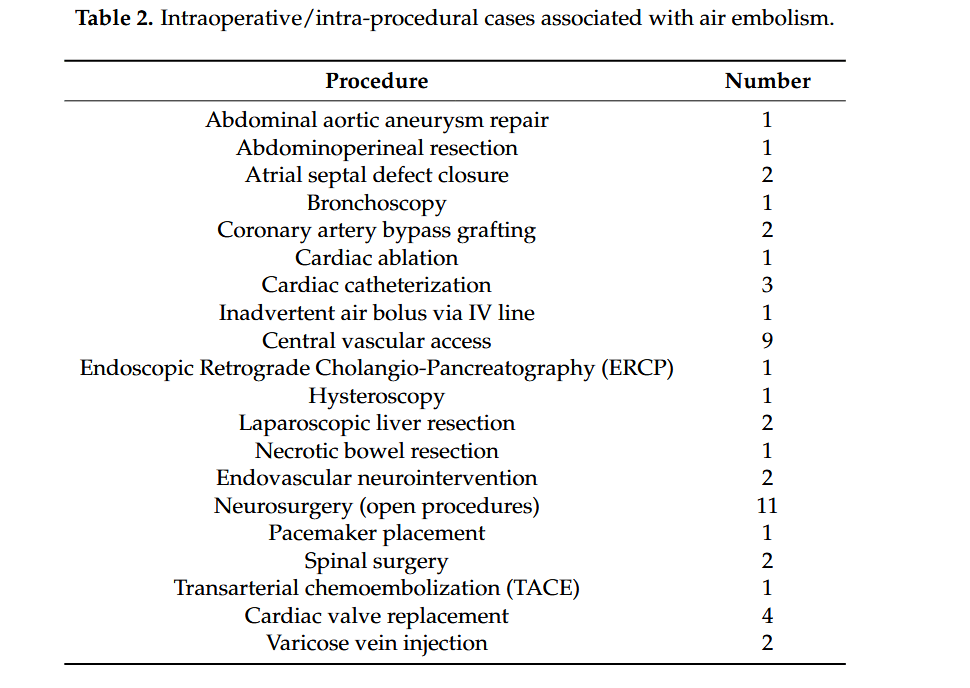
“Air embolism is a rare but potentially fatal complication of surgical procedures. Rapid recognition and intervention is critical for reducing morbidity and mortality.”
“Iatrogenic procedures are the main cause of vascular air embolism (VAE). This rare complication can arise in a wide range of clinical scenarios involving line placement, trauma, barotrauma, and several types of surgical procedures including cardiac, vascular, and neurosurgery. Traditionally, surgery and trauma were the most significant causes of systemic and cerebral air embolism; however, endoscopy, angiography, tissue biopsy, thoracocentesis, hemodialysis, and central/peripheral venous access now comprise a greater proportion. The insertion and maintenance of advanced vascular access devices are increasingly being performed within multiple clinical specialties. Moreover, the bulk of interventional radiology (IR) procedures commence with the placement of an intravascular sheath, which is a major risk factor for air embolism throughout the duration of the procedure. Endovascular procedures complicated by an intravascular air embolism result in significant morbidity and mortality. VAE is a potentially preventable condition, which arises as a result of a pressure gradient that allows air to enter the blood stream, which can subsequently cause blockages in blood flow. VAE has an estimated incidence of 1 in 772 according to one series, while another study found that the incidence of iatrogenic gas embolism complicates 2.65 per 100,000 hospitalizations; however, these figures are considered lower than the true incidence due to many unreported instances and undiagnosed asymptomatic patients.”
“There is a need for strategies to reduce the risk of ureteric injury, and to facilitate immediate recognition, during colorectal procedures. The preoperative placement of prophylactic ureteric stents or catheters has long been discussed as a technique that may assist colorectal surgeons in identifying and avoiding the ureters, and in recognising ureteric injury when it occurs. Debate surrounds this topic, however, with no consensus on the precise benefit of prophylactic ureteric stents, and some concerns regarding potential stent-related complications. Whilst the European Association of Urology (EAU) guidelines state that ‘visual identification of the ureters and meticulous dissection in their vicinity are mandatory to prevent ureteral trauma during abdominal and pelvic surgery’ (grade A recommendation), the use of ‘preoperative prophylactic stents’ are recommended only ‘in selected cases (based on risk factors and surgeon’s experience)’ (grade B). The American Society of Colon and Rectal Surgeons guidelines in surgery for diverticulitis state ‘ureteral stents are used at the discretion of the surgeon’ (grade 2C).
Table 4 Type of repair and outcomes of ureteric injuries