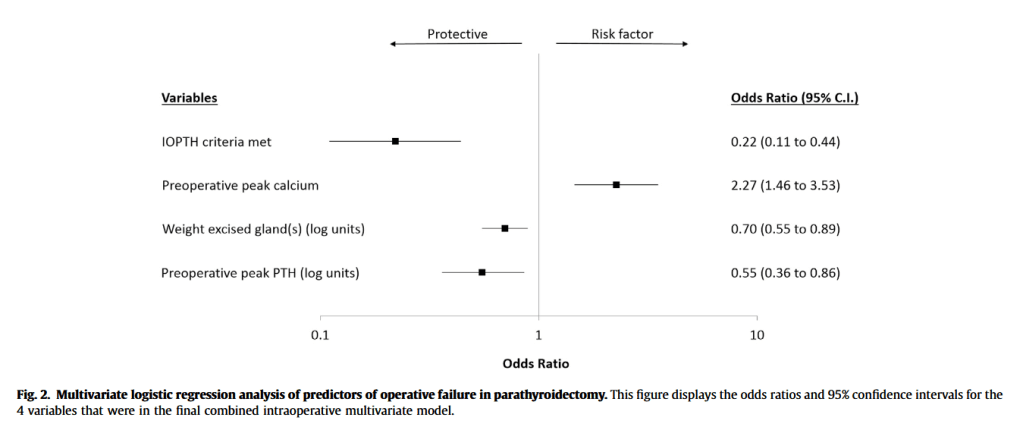
“Little is known about patient-level predictors of operative failure and persistent primary hyperparathyroidism (PHPT). Previous studies have attributed operative failure to inadequate preoperative imaging localization. Achievement of IOPTH criteria is a known predictor of operative success, though the final target IOPTH level is not agreed upon. Some researchers contend that final IOPTH levels should fall into the normal range, while others recommend lower levels. The independent contributions of preoperative localization, IOPTH biochemical cure, and preoperative biochemical severity to operative success are unclear. Better understanding of the relationship.”
“Right hemicolectomy is considered one of the simplest colorectal major procedures and is often considered an appropriate first step for residents and young fellows. Despite this, complications after right hemicolectomy for cancer are common, at ≈30%, and postoperative mortality is reported to be ≈3%. Anastomotic leak (AL) after right hemicolectomy for cancer is a major contributor to this short-term morbidity and mortality. The document AL rate after right hemicolectomy ranges widely, from 1.3% to 8.4%. This also has a significant impact on healthcare costs and major oncologic consequences, as demonstrated by the higher cancer recurrence rate after AL.”
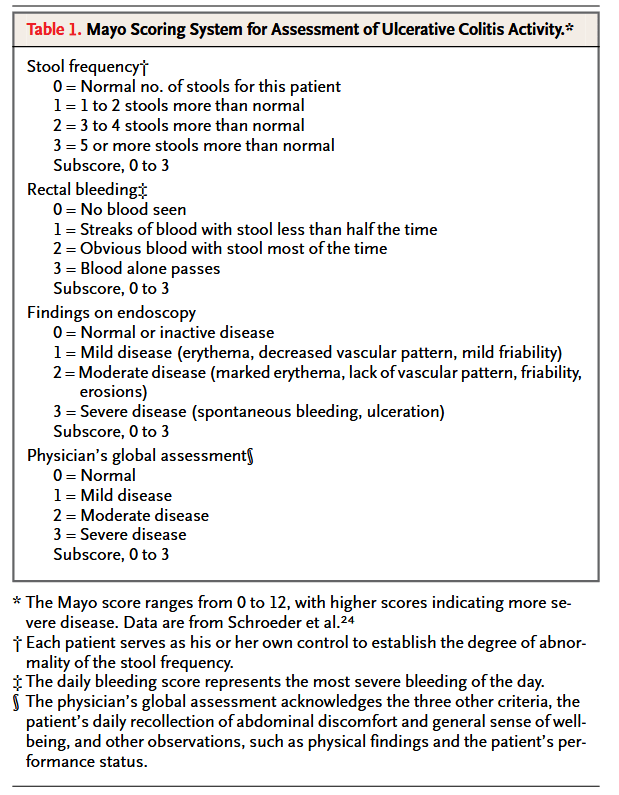
Ulcerative colitis is characterized by mucosal ulceration, rectal bleeding, diarrhea, and abdominal pain. Pharmacologic management of ulcerative colitis has relied mainly on 5-aminosalicylates, corticosteroids, and immunosuppressants, including purine antimetabolites and cyclosporine. Corticosteroid dependence is a clinically important problem; furthermore, the probability of colectomy within the first five years after diagnosis ranges from 9 percent in patients with distal colitis to 35 percent in patients with total colitis, most commonly because of failed medical therapy. The cumulative risk of recurrent inflammatory bowel disease in the form of pouchitis ranges from 15.5 percent one year after the procedure to 45.5 percent 10 years after the procedure. Accordingly, new treatments for ulcerative colitis are needed.”
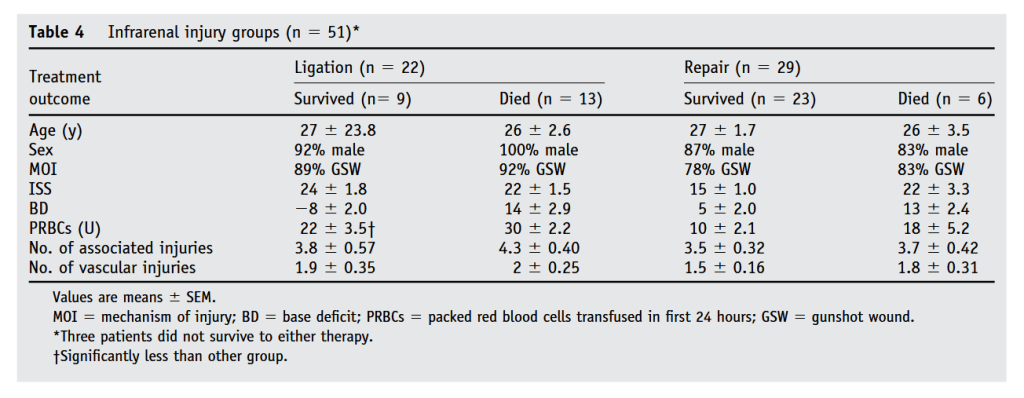
“Injury to the inferior vena cava (IVC) is a relatively rare event occurring more commonly after penetrating trauma (.5%–5%) than after blunt trauma (.6%–1%). The incidence of IVC injuries, however, has been increasing in civilian trauma centers, with these injuries accounting for up to 40% of abdominal vascular injuries in recent series. Because of the increasing frequency and persistently high mortality associated with these injuries, perioperative management of the IVC remains a focus of interest. Indeed, while ligation of the significantly injured IVC is an acceptable practice in the era of damage control surgery, little long-term follow-up data are available in survivors of this technique.”
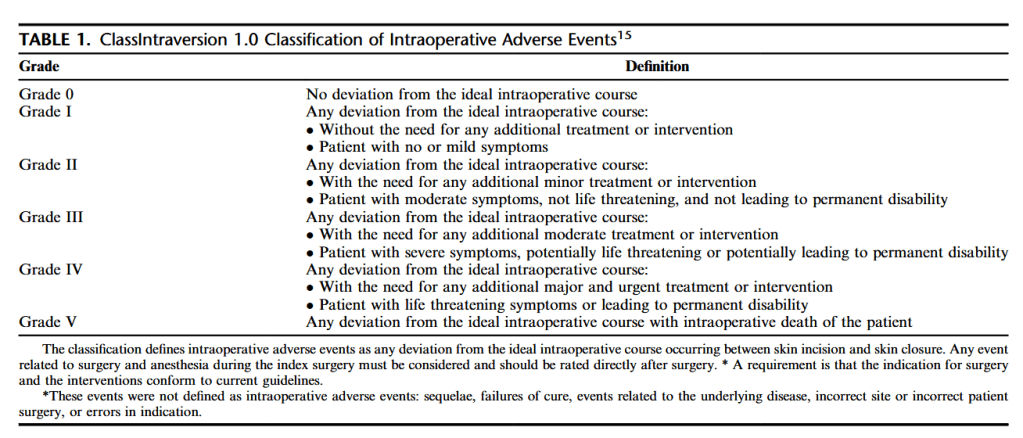
“In surgery, adverse events and medical errors occur pre-operatively, intraoperatively, and postoperatively. Standardized classification of postoperative complications, for example, using the Clavien-Dindo classification, is widely adopted, and has proven relevant to research and quality improvement programs. Prospectively validated classification systems for intraoperative adverse events (iAEs) are not yet broadly adopted. IAEs have a major impact at many levels. First, there is an association between iAEs and postoperative outcome. Second, hospital stays for patients experiencing iAEs are 40% more expensive compared with patients without iAEs. Third, readmission rates in patients whose surgery is complicated by an iAE are twofold higher. Recently a promising new and practical classification system for iAEs was proposed, the classification of intraoperative complications (CLASSIC). CLASSIC defines iAEs as any deviation from the ideal intraoperative course occurring between skin incision and skin closure, irrespective of the origin (ie, surgical and anesthesiological difficulties, or technical failures). Compared with previous scores such as the severity score by Kaafarani et al. ClassIntra is more inclusive, accounting for any type iAE, for example, surgical, anesthesiologic, and organizational, and can be graded directly after skin closure.”
“Colorectal cancer is the second-leading cause of cancer-related mortality in both the United States and Europe. With respect to prognosis, increasing evidence has suggested that systemic inflammation is a key predictor of disease progression and survival for colorectal cancer patients undergoing surgery. Furthermore, whereas red blood cell (RBC) transfusions may be life-saving in some circumstances, there has been growing evidence that transfusions are associated with adverse postoperative outcomes, including infectious complications and cancer recurrence. These detrimental effects are thought to be related to systemic inflammation and transfusion-related immunomodulation (TRIM). Whereas the exact mechanisms remain unknown, TRIM seems to be related to various immunologic changes, including decreased interleukin (IL)-2 production, monocyte and cytotoxic cell activity inhibition, increased suppressor T-cell activity, and immunosuppressive prostaglandin release.”
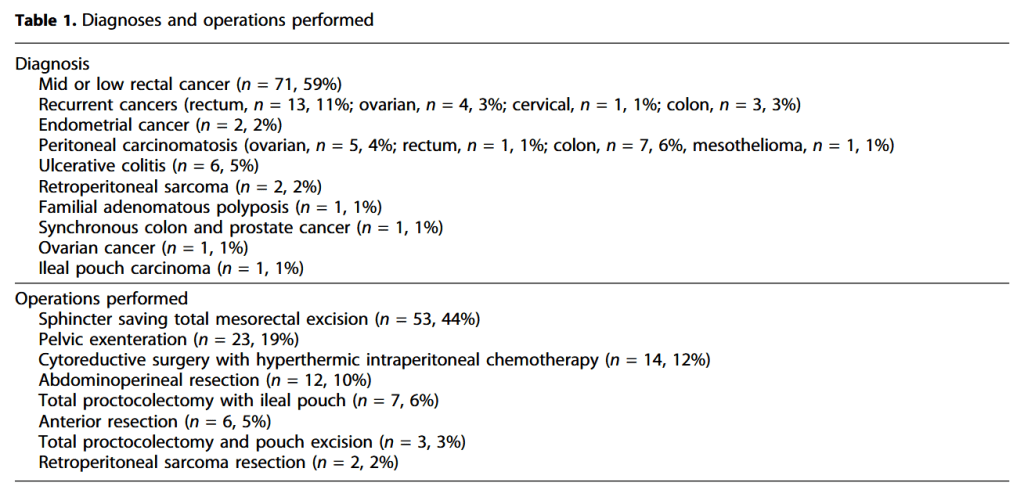
“Complex abdominopelvic surgery (CAPS) includes a wide variety of difficulties related to primary disease and hostile intrapelvic environment. Any radical abdominopelvic operation which is not standardized is complex. Hence, radical oncologic operations for the primary advanced or recurrent carcinoma of pelvic organs, revisional operations for failed restorative operations for maintaining intestinal continuity are considered as CAPS.”