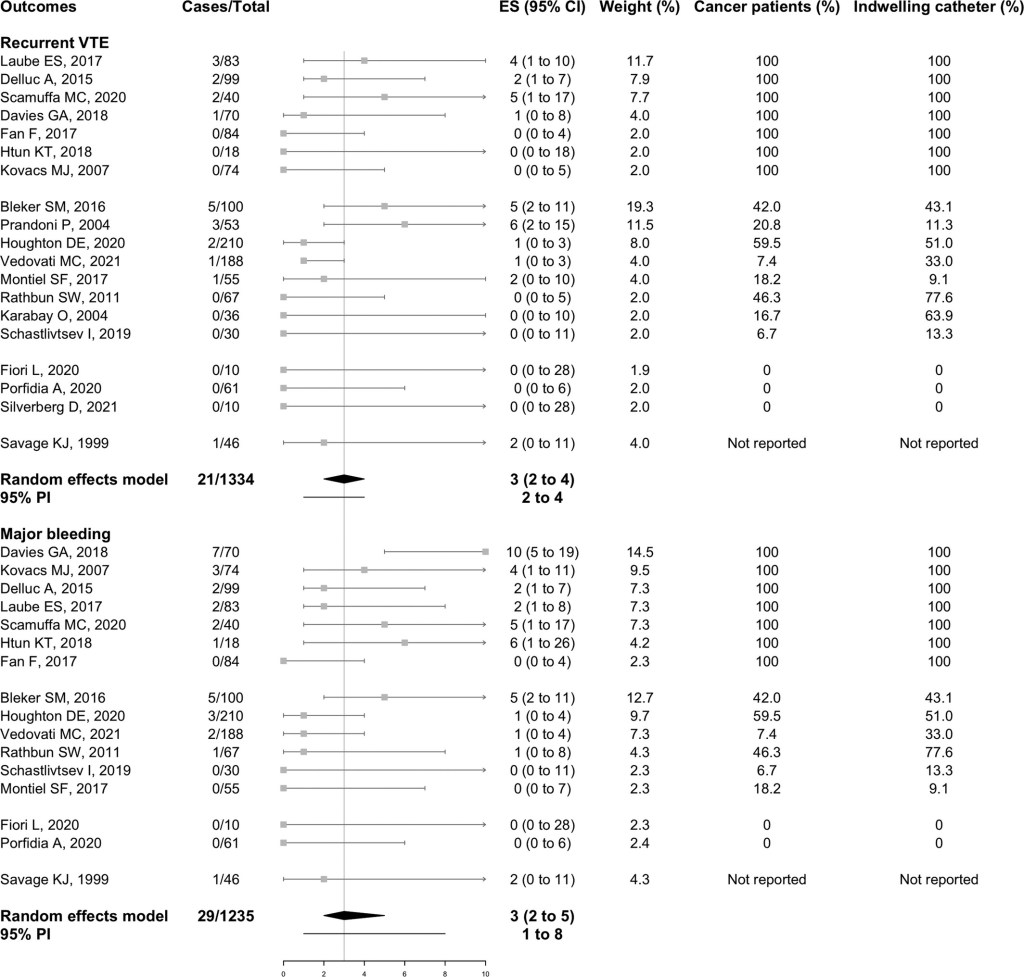
“Upper extremity DVT may be complicated by recurrent thrombosis in about 7.5% of cases and by post-thrombotic syndrome in 19.4% of cases, with higher rates of recurrence in patients with cancer-associated thrombosis and of post-thrombotic syndrome in patients with unprovoked thrombosis or related to congenital or anatomical abnormalities. The intensity and duration of anticoagulant treatment need to be balanced against the risk of bleeding
complications, especially in high-risk subgroups like patients with cancer in whom major bleeding events were reported in up to 10%.”