“There is evidence of endothelial dysfunction and a dysregulation of coagulation and fibrinolysis in individuals with HIV. In a study of 109 HIV-infected patients with advanced disease, 10% developed venous thrombosis and 6% developed arterial thrombosis. A variety of laboratory abnormalities were reported, including protein C deficiency, increased factor VIII concentrations, high fibrinogen concentrations, and free protein S deficiency. HIV infection is also associated with an increased D-dimer level, which suggests that HIV infection might be associated with a pro-thrombotic state. HIV disease is theorized to produce a pro-thrombotic state through mechanisms related to activation of the innate and adaptive immune system by low level HIV replication, co-pathogens, and microbial products trans-located from the gastrointestinal tract,”
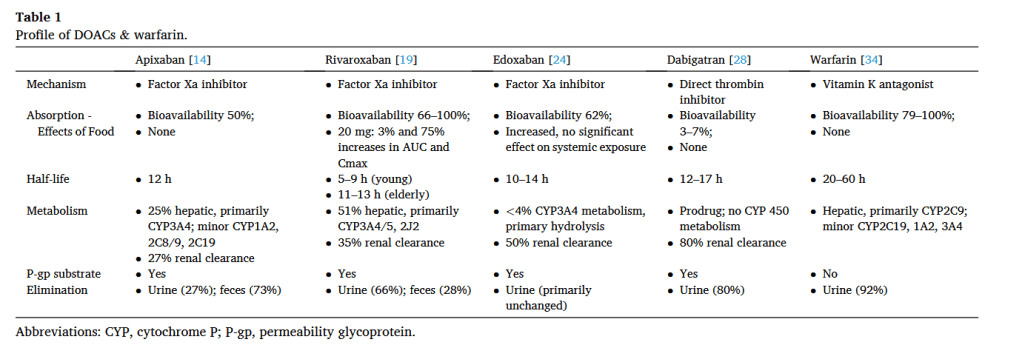
“The impact of HAART on coagulation is unclear. Protease inhibitors (PI) have been associated with higher fibrinogen levels and lipodystrophy. PIs are also thought to interfere with cytochrome P (CYP) 450 metabolism and regulation of thrombotic proteins. This may cause a pro-thrombotic state in HIV-infected individuals”
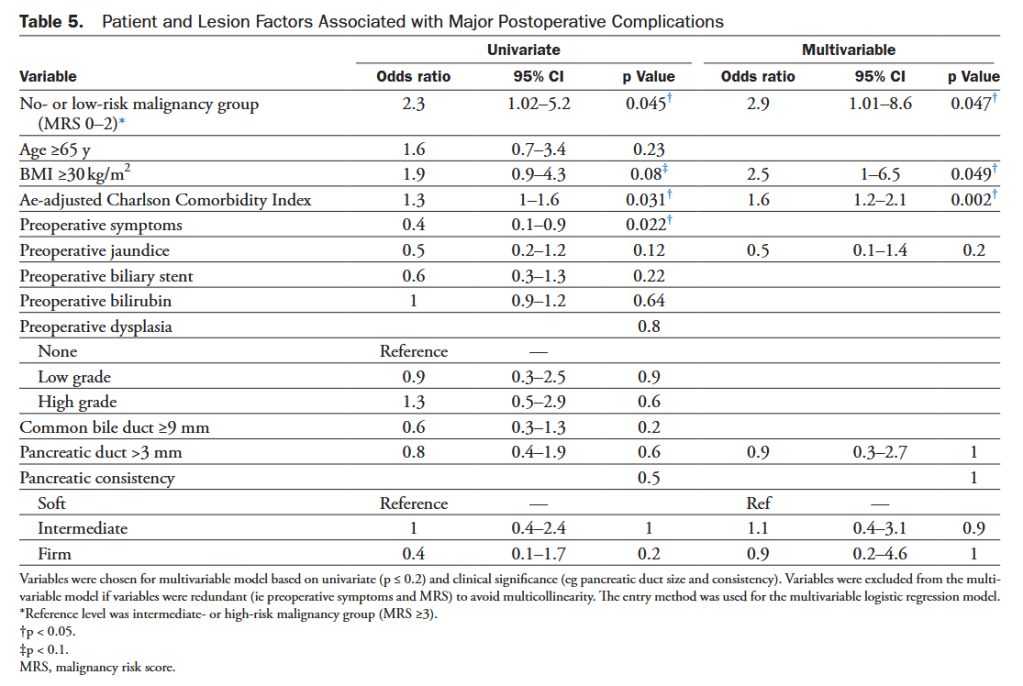
“Preoperative assessment of underlying malignancy in non-FAP-related PAs requiring PD may be difficult, as endoscopic biopsy carries a false-negative rate as high as 50%. Although PD aims at preempting malignant transformation through complete removal of DA, it comes with significant morbidity and mortality risks. This is particularly relevant in patients with benign or premalignant pathology due to soft pancreatic parenchymal texture and small pancreatic duct diameter.”
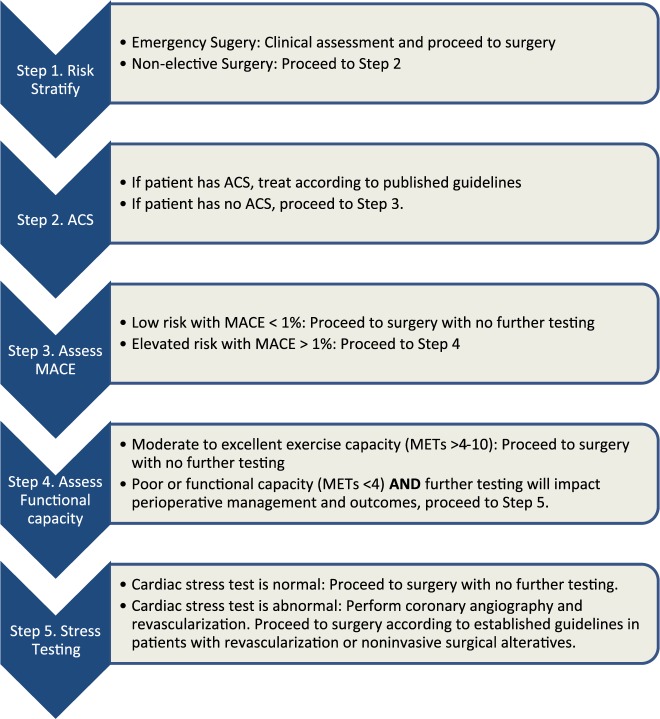
A stepwise approach to perioperative cardiac assessment assists clinicians in determining when surgery should proceed or when a pause for further evaluation is warranted.
2.
Cardiovascular screening and treatment of patients undergoing noncardiac surgery should adhere to the same indications as nonsurgical patients, carefully timed to avoid delays in surgery and chosen in ways to avoid overscreening and overtreatment.
3.
Stress testing should be performed judiciously in patients undergoing noncardiac surgery, especially those at lower risk, and only in patients in whom testing would be appropriate independent of planned surgery.
4.
Team-based care should be emphasized when managing patients with complex anatomy or unstable cardiovascular disease.
5.
New therapies for management of diabetes, heart failure, and obesity have significant perioperative implications. Sodium-glucose cotransporter 2 inhibitors should be discontinued 3 to 4 days before surgery to minimize the risk of perioperative ketoacidosis associated with their use.
6.
Myocardial injury after noncardiac surgery is a newly identified disease process that should not be ignored because it portends real consequences for affected patients.
7.
Patients with newly diagnosed atrial fibrillation identified during or after noncardiac surgery have an increased risk of stroke. These patients should be followed closely after surgery to treat reversible causes of arrhythmia and to assess the need for rhythm control and long-term anticoagulation.
8.
Perioperative bridging of oral anticoagulant therapy should be used selectively only in those patients at highest risk for thrombotic complications and is not recommended in the majority of cases.
9.
In patients with unexplained hemodynamic instability and when clinical expertise is available, emergency focused cardiac ultrasound can be used for perioperative evaluation; however, focused cardiac ultrasound should not replace comprehensive transthoracic echocardiography.”
Stepwise Approach to Perioperative Cardiac Assessment ∗Cardiovascular risk factors: hypertension, smoking, high cholesterol, diabetes, women age >65 y, men age >55 y, obesity, family history of premature CAD. †Determining elevated calculated risk depends on the calculator used. Traditionally, RCRI >1 or a calculated risk of MACE with any perioperative risk calculator >1% is used as a threshold to identify patients at elevated risk. §Abnormal biomarker thresholds: troponin >99th percentile URL for the assay; BNP >92 ng/L, NT-proBNP ≥300 ng/L. ‡Conditions that pose additional risk for MACE. ‖Noninvasive stress testing or CCTA suggestive of LM or multivessel CAD. Colors correspond to Class of Recommendation in Table 3. BNP indicates B-type natriuretic peptide; CABG, coronary artery bypass grafting; CAD, coronary artery disease; CCTA, coronary computed tomography angiography; CIED, cardiovascular implantable electronic device; CVD, cardiovascular disease; DASI, Duke Activity Status Index; ECG, electrocardiogram; GDMT, guideline-directed management and therapy; ICD, implantable cardioverter-defibrillator; LM, left main; MACE, major adverse cardiovascular event; METs, metabolic equivalents; NCS, noncardiac surgery; NT-proBNP, N-terminal pro b-type natriuretic peptide; RCRI, Revised Cardiac Risk Index; and URL, upper reference limit.Continue reading →
“The main purpose of perioperative cardiac evaluation involves answering few basic questions. What are the underlying cardiac risk factors which a patient might have before s/he undergoes noncardiac surgery? Will such cardiac evaluation change the management of the patient? Will it defer surgery altogether in favor of resolving the patient’s cardiac disease and hence reducing perioperative mortality? What will be the course of management in the postoperative period? Communication among the complete medical team involved in patient care, including the internist, cardiologist, anesthesiologist, surgeon, and ancillary staff, is of utmost importance, along with the facilitation of shared decision making by the patient.”
Algorithm for perioperative cardiac risk assessment prior to noncardiac surgery.Continue reading →
“A surgical site infection (SSI) is defined as an infection of the incision (superficial SSI), the tissue below the incision (deep SSI), or within the abdominal cavity (organ space SSI). SSI accounts for more than 20% of all health care-associated infections and is the most common infection after surgery, affecting an estimated 300,000 patients annually. Compared with other surgical subspecialties, patients undergoing colorectal surgery are at the highest risk for developing an SSI with an estimated incidence of 5% to 30%. Patients undergoing emergency colorectal surgery with colon perforation have an SSI incidence as high as 80%.”
TABLE 2.
Summary and strength of GRADE recommendations for preventing SSIs
Summary
Recommendation strength
GRADE quality of evidence
1
Implementing an SSI bundle for patients undergoing colorectal surgery can decrease the incidence of SSI
Strong
Moderate
2
Oral antibiotics in combination with mechanical bowel preparation have been shown to decrease the incidence of SSI after elective colorectal resection
Strong
Moderate
3
In circumstances where a mechanical bowel preparation is contraindicated or otherwise omitted, preoperative oral antibiotic preparation alone can reduce the incidence of SSI
Conditional
Moderate
4
Showering with chlorhexidine before colorectal surgery does not significantly impact SSI rates
Strong
Moderate
5
Smoking cessation before surgery may be recommended to reduce the risk of SSI
Conditional
Moderate
6
On the day of colorectal surgery, patients should have their hair removed from the surgical site using a clipper or not removed at all. Shaving with a razor before surgery is discouraged
Strong
Moderate
7
Patients undergoing colorectal resection should have parenteral antibiotics administered within 60 min of incision. Dosing and redosing should be based on the pharmacokinetic profile of the antibiotic
Strong
Low
8
Patients who report a penicillin allergy may be evaluated for having true hypersensitivity and high-risk reactions to penicillin. Delabeling a penicillin-allergic patient can facilitate the appropriate use of a preoperative prophylactic beta-lactam antibiotic and improve outcomes
Conditional
Low
9
For most clean and clean-contaminated cases, prophylactic parenteral antibiotics should be limited to the initial 24 h postoperatively
Strong
Moderate
10
Cleansing the surgical site with chlorhexidine–alcohol-based preparation is typically recommended for patients undergoing colorectal surgery
Strong
Moderate
11
Hyperglycemia on the day of surgery and in the immediate postoperative period may increase the risk of SSI after elective colorectal resection
Conditional
Moderate
12
Maintaining intraoperative normothermia may decrease the incidence of SSI in patients undergoing colorectal surgery
Conditional
Low
13
High-fractionated oxygen is not routinely recommended to prevent SSI
Conditional
Moderate
14
Wound protectors can decrease the incidence of SSI after colorectal surgery
Strong
High
15
Minimally invasive colorectal surgery can decrease the incidence of SSI compared to open surgery
Strong
High
16
Topical antimicrobial agents applied to the surgical incision are not recommended
Strong
Low
17
NPWT for primarily closed incisions may decrease the incidence of SSI
Conditional
Moderate
18
Advanced silver or antimicrobial dressings are not routinely recommended for clean or clean-contaminated wounds after colorectal surgery
Conditional
Moderate
GRADE = Grading of Recommendations, Assessments, Development, and Evaluation; NPWT = Negative pressure wound therapy; SSI = surgical site infection.
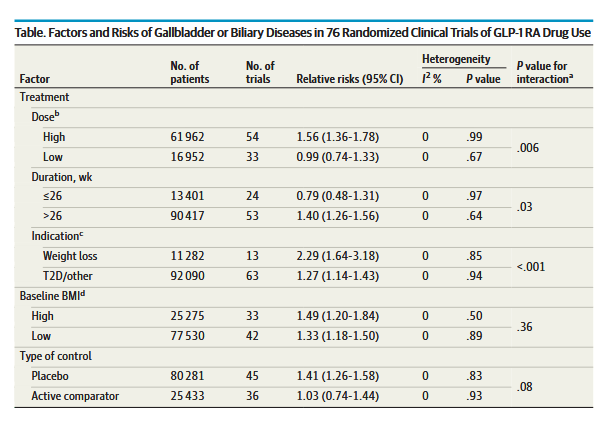
“Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) are recommended for patients with type 2 diabetes to control glycemia and reduce cardiovascular risk, and for patients with obesity to reduce weight. Given the wide-spread use of these drugs, potential safety concerns deserve attention. Several randomized clinical trials (RCTs) have shown a higher rate of gallbladder disorders in patients who were randomized to GLP-1 RAs vs a placebo. However, whether increased risk of gallbladder-related events is a class effect of GLP-1 RAs has not been established, and prescribing information for all GLP-1 RA medications does not provide a warning regarding increased risk of gallbladder disorders. In addition to gallbladder-related events, a post hoc analysis of the LEADER trial 8 found significantly increased risks of acute biliary obstruction in patients randomized to liraglutide compared with placebo. Because GLP-1 RAs are generally prescribed at higher doses for weight loss rather than for control of type 2 diabetes, there may be differential effects on risk for gallbladder or biliary diseases depending on dose.”
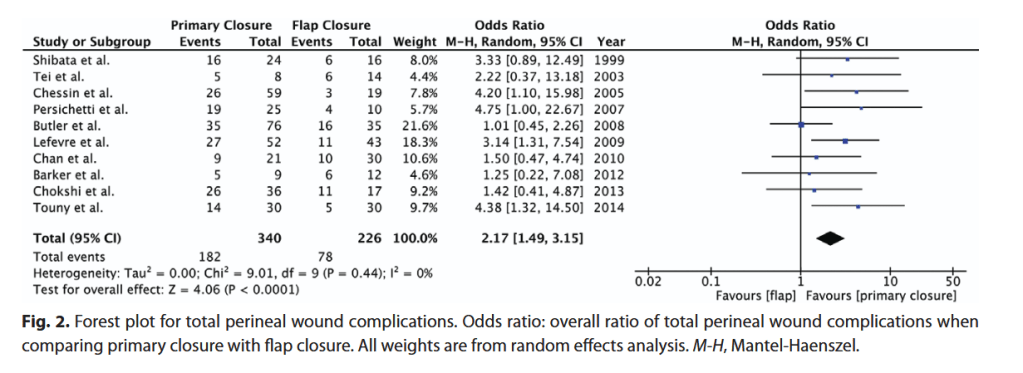
“Abdominoperineal resection and pelvic exenteration for resection of malignancies can lead to large perineal defects with significant surgical-site morbidity. Myocutaneous flaps have been proposed in place of primary closure to improve wound healing. A systematic review was conducted to compare primary closure with myocutaneous flap reconstruction of perineal defects following abdominoperineal resection or pelvic exenteration with regard to surgical-site complications.”