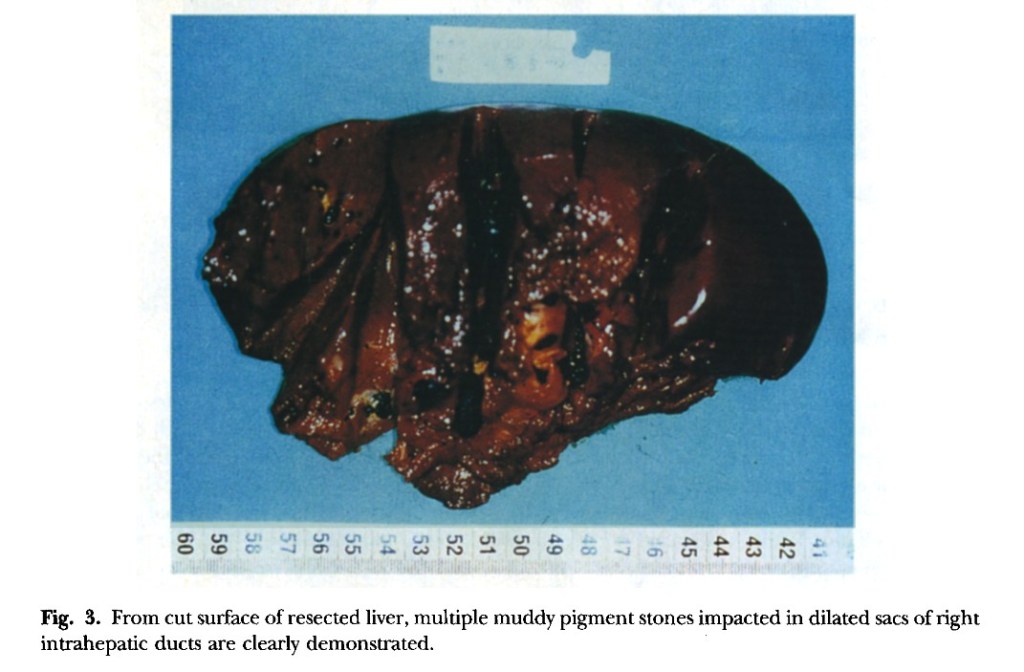
“Hepatic resection has been thought to he the most effective treatment modality for selected patients who have left-sided hepatolithiasis and meet the criteria of resection.” Under the same criteria the role of right hepatic resection, especially right hepatic lobectomy, is still ambiguous for patients who have right-sided hepatolithiasis because of the higher operative risk. This report presents the results of right hepatic lobectomy in the treatment of patients with right-sided hepatolithiasis after careful selection. In particular, we focus on the rationale and indications for this procedure,”
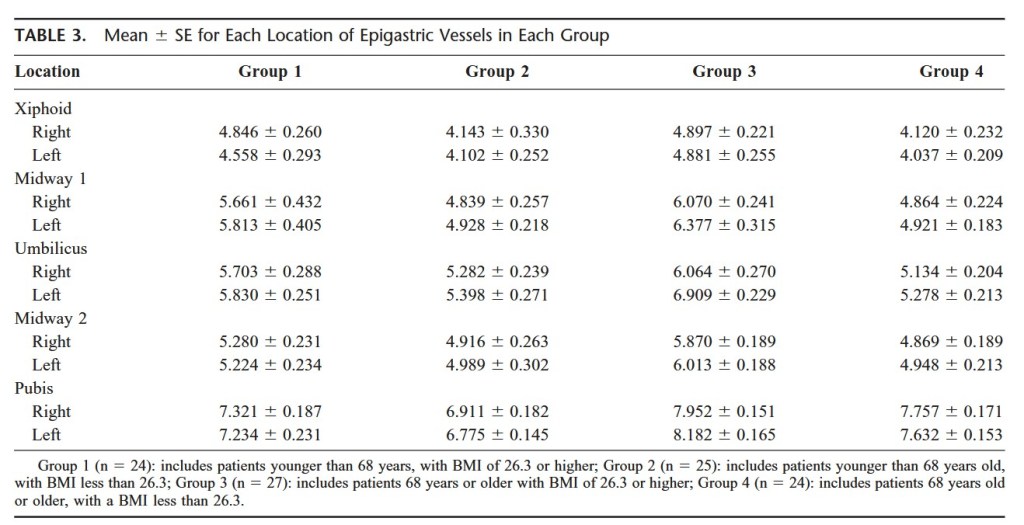
“Trauma to abdominal wall blood vessels occurs in 0.2% to 2% of laparoscopic procedures. Both superficial and deep abdominal wall vessels are at risk. The superficial vessels may be located by transillumination; however, the deep epigastric vessels cannot be effectively located by transillumination and, thus, other techniques should be used to minimize the risk of injury to these vessels.”
“The development of an anastomotic stricture at the site of the gastrojejunostomy following Roux-en-Y gastric bypass (RYGBP) is associated with substantial morbidity. Various techniques are available for creating the gastrojejunal anastomosis, including hand-sewing and using a circular or linear stapler, to reduce complication rates. The aim of this study was to assess the incidence of gastrojejunal anastomotic strictures in patients who underwent antecolic antegastric Roux-en-Y gastric bypass (AA-RYGBP) with the use of a linear stapler and to evaluate the outcomes of endoscopic pneumatic dilatation as a treatment option for patients with anastomotic stricture.”
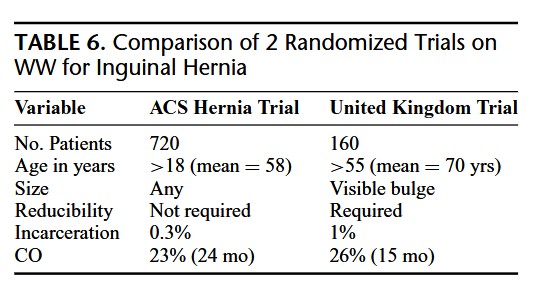
“Annually, more than 20 million inguinal herniorrhaphies are performed worldwide, and it is one of the most common operations performed by general surgeons. Up to one third of patients with inguinal hernias are asymptomatic or minimally symptomatic at the time of presentation. Historically, surgeons have recommended repair of an inguinal hernia at diagnosis even if minimally symptomatic to avoid a hernia accident, which is defined as a bowel obstruction caused by the hernia or strangulation of the contents of the hernia, or both. However, on the basis of the results of 2 recent randomized clinical trials (RCTs), one conducted in the United Kingdom and the other in North America, watchful waiting (WW) has now become an accepted alternative to routine repair. In 2011, the longer-term results of the United Kingdom trial were published. Using Kaplan-Meier analysis, 72% of patients were predicted to crossover (CO) from WW to surgery by 7.5 years causing the authors to conclude that routine repair should be recommended for minimally symptomatic patients without medical contraindications to surgery.”
“The results of this study show that WW remains a safe strategy even on long-term follow-up. However, patients who present to their physicians to have the hernia evaluated, especially if they are elderly, should be informed that they will almost certainly come to surgery eventually. These results should not be extrapolated to the broader population of all patients with asymptomatic or minimally symptomatic hernias.”
“Rates of postoperative bleeding and transfusion are either widely variable or often unreported. As a high-volume center, we have anecdotally appreciated significant rates of each but admittedly have not accurately reported the degree of this specific morbidity in our practice. This study aims to quantify postoperative blood loss, rates of blood transfusion, and the incidence of operative or endovascular intervention for bleeding, as well as associated risk factors contributing to this morbidity in patients undergoing open TAR.”
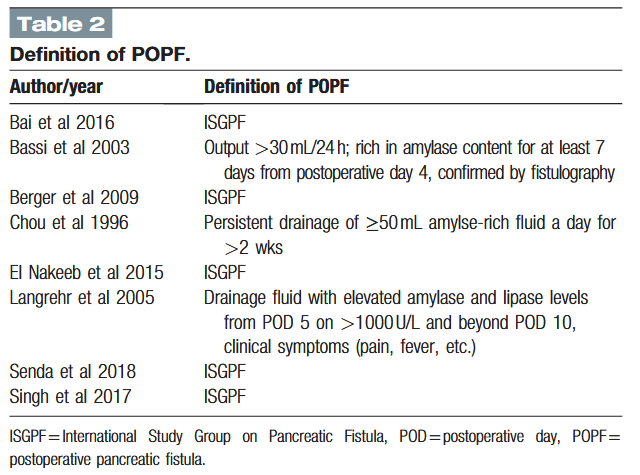
“Pancreaticoduodenectomy (PD) is a complex, high-risk standard surgical procedure that is indicated primarily for periampullary diseases. Central to the entire discipline of PD are postoperative mortality and morbidity. Although operative mortality in patients undergoing PD has decreased, the incidence of postoperative morbidity remains high at 40% to 50%. Postoperative pancreatic fistula (POPF) is the most common complication, with rates ranging from 5% to 30% in previous studies. Many methods have been described to decrease the risk of POPF, including the use of medications (prophylactic octreotide, sealants), prophylactic pancreatic stenting, and improvements in pancreatic reconstruction techniques. The most commonly used pancreatic reconstruction techniques are pancreaticogastrostomy (PG) and pancreaticojejunostomy (PJ).”
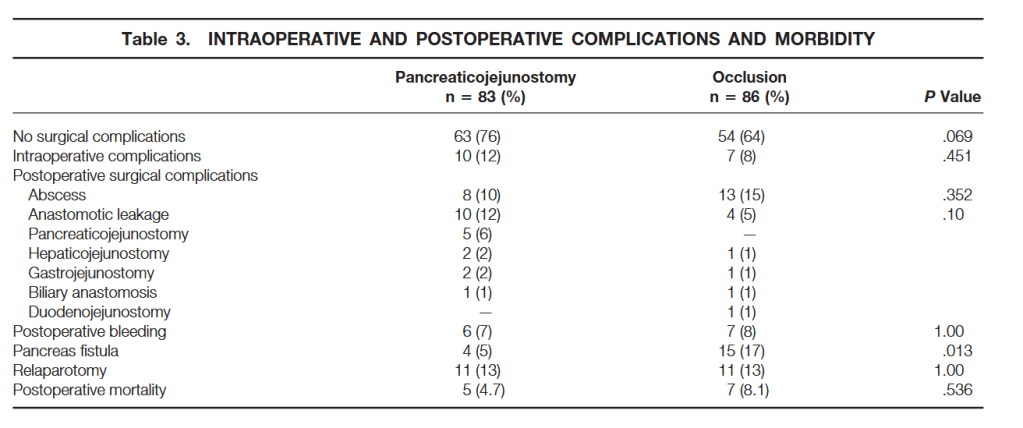
“Pancreatic fistulas and pancreatitis may develop in the pancreatic remnant and may lead to hemorrhage, sepsis, and subsequent death. Procedures to avoid pancreaticojejunostomy were described, including total pancreatectomy. None of these has so far proven to diminish morbidity significantly. Another technique investigated is obliteration closure of the pancreatic duct with a chemical substance, thus avoiding a pancreaticojejunostomy. This method was proposed by Gebhardt et al. They studied the effect of occlusion of the pancreatic duct system with Ethibloc, an alcoholic prolamine, in animal experiments. The pancreatic duct may also be occluded with a fibrin glue solution, Tissucol, which was found to have a more protective effect on beta cell function than the other solutions used.”