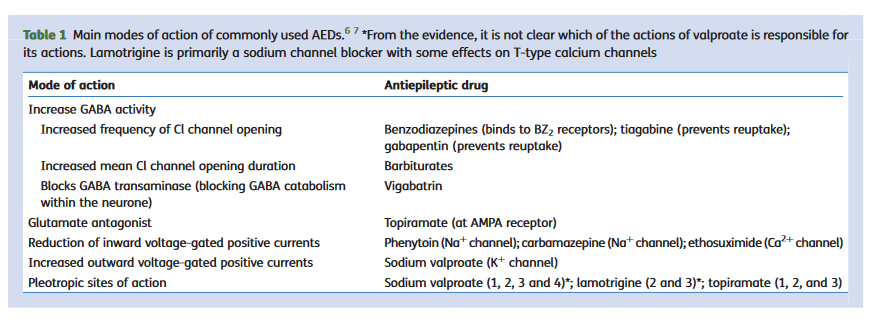
“Epilepsy is the most common serious neurological disorder, with a prevalence of 0.5–1% of the population. Anaesthetists are frequently faced with patients with epilepsy undergoing emergency or elective surgery and patients suffering seizures and status epilepticus in the intensive care unit (ICU).”
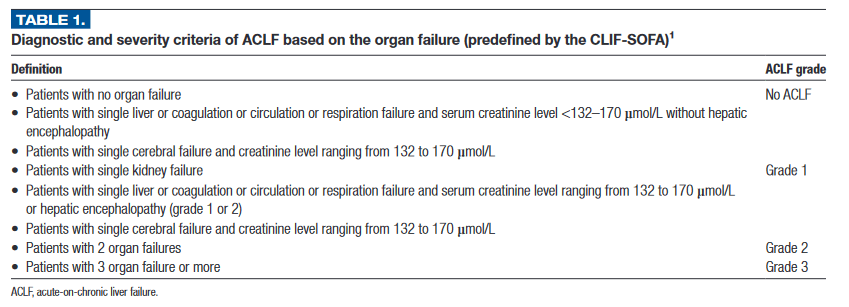
“Liver transplantation (LT) has revolutionized the treatment of cirrhotic patients. However, access to transplant is limited as demand for organs exceeds availability. Current allocation gives the highest priority to patients with the highest mortality risk. Hence, several patients awaiting LT may deteriorate while waiting for LT.”
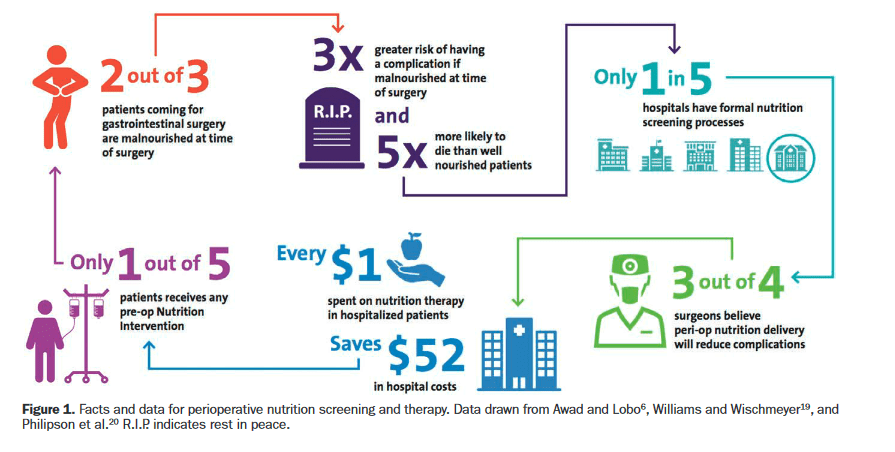
“Perioperative malnutrition has proven to be challenging to define, diagnose, and treat. Despite these challenges, it is well known that sub-optimal nutritional status is a strong independent predictor of poor postoperative outcomes.”
“Malnourished surgical patients have significantly higher postoperative mortality, morbidity, length of stay (LOS), readmission rates, and increased hospital costs.It is estimated that 24%–65% of patients undergoing surgery are at nutrition risk. Additionally, recent prospective observational data indicate that undernourished patients or patients at risk of malnutrition are twice as likely to be readmitted within 30 days after elective colorectal surgery.”
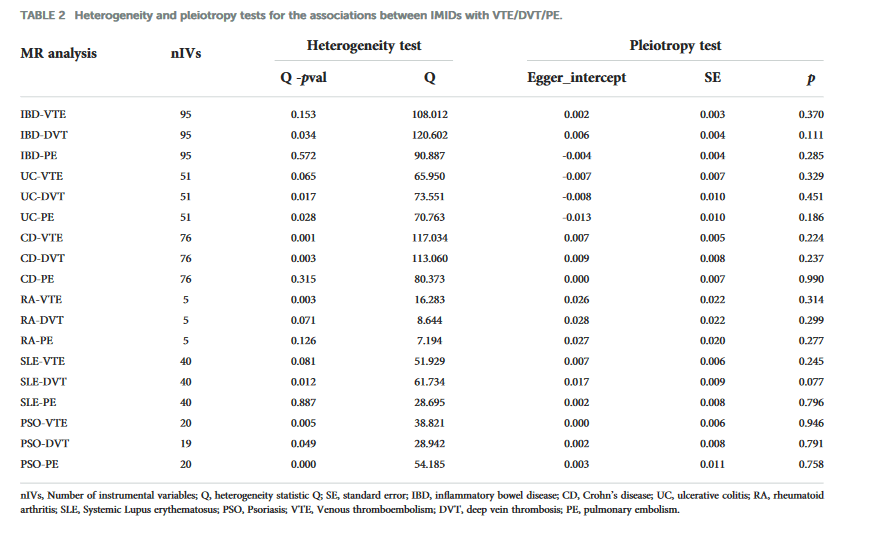
“Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), affects ~10 million people worldwide every year, representing the third most common cardiovascular disease globally. The 30-day case fatality rate after VTE diagnosis is 10.6%, with about 30% to 50% of survivors developing long-term complications that increase the burden of this disease.”
“Thrombosis is the most feared complication of cardiovascular diseases and a main cause of death worldwide, making it a major health-care challenge. Platelets and the coagulation cascade are effectively targeted by antithrombotic approaches, which carry an inherent risk of bleeding. Moreover, antithrombotics cannot completely prevent thrombotic events, implicating a therapeutic gap due to a third, not yet adequately addressed mechanism, namely inflammation.”
“An increased risk of DVT and PE in patients with IBD has been evident for the past 75 years. Most work in this area has not looked specifically at patients undergoing surgery. Patients with IBD frequently require surgical intervention, and an understanding of their risk of venous thromboembolism is therefore an important issue. This study aimed to examine rates of DVT and PE in patients with IBD undergoing surgery using data from the NSQIP.”
‘Clostridium perfringens is one of the most widely dispersed opportunistic pathogens and is well known to produce a number of toxins to cause several forms of histotoxic and enteric diseases in humans and animals [2]. Based on the production of four major toxins i.e., alpha, beta, epsilon and iota, it is categorized into five toxin-types viz. A, B, C, D and E. While it is ambiguous why C. perfringens produces so many diverse toxins, it is well known that it uses chromosomally-encoded α-toxin (which has phospholipase C (plc) and sphingomyelinase activities with hemolytic, necrotic and lethal abilities) as a chief virulent factor and key mediator for most of C. perfringens-associated diseases.”
Standard curves representing the quantitative detection of reference strains of C. perfringens by Amp-qPCR assay. C. perfringens ATCC 13124T, ATCC 9856, ATCC 3624, ATCC 3626, ATCC 12917, ATCC 14809, ATCC 27324, and CS 052–1 were cultivated separately in Glu-mGAM. DNA fractions were extracted from the culture samples in the early stationary phase (24 h), and bacterial counts were determined microscopically with DAPI staining. 10-fold serial dilutions of DNA corresponding to the bacterial counts ranging from 100 to 105 bacterial cells were assessed by 16S rRNA gene-specific a, plc-specific b, and cpe-specific c Amp-qPCR assays. The Cq values obtained were plotted against the log10number of bacterial cells subjected to each reaction. Data are expressed as means and standard deviations of the results from 7 strains (ATCC 13124T, ATCC 9856, ATCC 3624, ATCC 3626, ATCC 12917, ATCC 14809, and ATCC 27324) in the 16S rRNA gene-specific and plc-specific primer sets, and 3 strains (ATCC 12917, ATCC 14809, and CS 052–1) in the cpe-specific primer set