“Resections of the pancreas reaching to the left of the superior mesenteric vein are defined as distal pancreatectomy. Most distal pancreatectomies are done electively (84%) as a result of chronic pancreatitis (24%), other benign diseases (22%), malignant diseases (18%), neuroendocrine tumours (14%), and pancreatic pseudocysts (6%). The remaining 16% are emergency cases after abdominal trauma or miscellaneous pathological
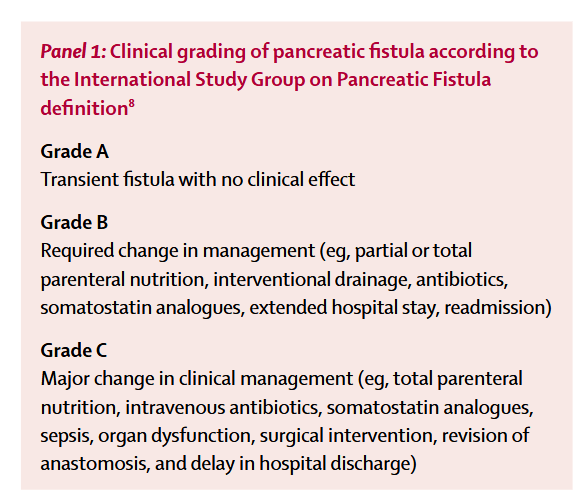
diagnoses. A systematic review supports the evidence that postoperative pancreatic fistula formation represents a major source of postoperative morbidity (13–64%) and is associated with several further complications, such as intra-abdominal abscess, wound infection, sepsis, malabsorption, and haemorrhage.
A meta-analysis of the most favoured and reported techniques (stapler trans-section and closure vs scalpel trans-section and hand-sewn closure of the pancreatic remnant) did
not define the optimum surgical technique of pancreatic stump closure. Therefore, the multicentre randomised DISPACT trial was designed to assess the effect of stapler
versus hand-sewn closure on formation of postoperative pancreatic fistula after distal pancreatectomy.”