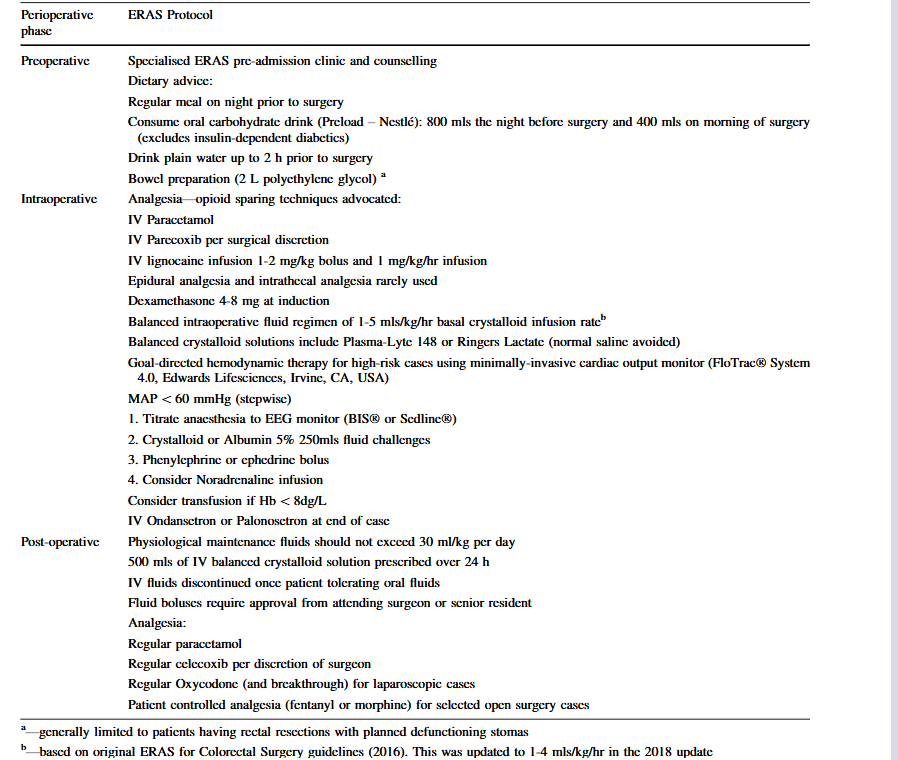
“Acute kidney injury (AKI) is a common complication following major abdominal surgery and is associated with increased length of hospital stay, the progression of chronic kidney disease (CKD), and increased long-term mortality. The rate of AKI amongst patients within different enhanced recovery programs (ERP) is reported to be between 3 and 23%. Patient-related risk factors for AKI include age, comorbidities such as hypertension and diabetes, a history of CKD, and use of angiotensin-converting enzyme inhibitors. Procedure-related factors that may impact on the prevalence of AKI include open surgery, the requirement for blood products, the use of intraoperative vasopressors, and a restrictive perioperative fluid regimen. The original guidelines published by the Enhanced Recovery After Surgery (ERAS) Society for colorectal surgery (CRS) as well as their recent update (2018 guidelines) promote a number of measures which aim to maintain near euvolaemia such as preoperative carbohydrate loading, avoidance of bowel preparation, minimisation of fasting times, minimally invasive surgery, and early resumption of oral fluid therapy.”